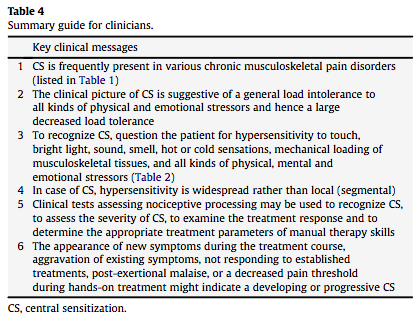
Viktig studie om nervesystemet og bindevevets «adhesions» som bidragsyter til smerte.
http://www.frontiersin.org/Integrative_Physiology/10.3389/fphys.2013.00115/full
«Work by Brieg, Sunderland, and others has emphasized the ability of the nervous system to undergo accommodative changes in length in response to the range of limb and trunk movements carried out during daily activity. If that ability to elongate is impaired—due to movement restrictions in tissues adjacent to nerves, or due to swelling or adhesions within the nerve itself—the result is an increase in mechanical tension within the nerve. »
«This adverse neural tension, also termed neurodynamic dysfunction, is thought to contribute to pain and other symptoms through a variety of mechanisms. These include mechanical sensitization and altered nociceptive signaling, altered proprioception, adverse patterns of muscle recruitment and force of muscle contraction, reduced intra-neural blood flow, and release of inflammatory neuropeptides. »

«In our clinical work, we have found that neuromuscular restrictions are common in CFS, and that many symptoms of CFS can be reproduced by selectively adding neuromuscular strain during the examination.»
«As defined by Yunus, central sensitivity is “clinically and physiologically characterized by hyperalgesia (excessive sensitivity to a normally painful stimulus, e.g., pressure), allodynia (painful sensation to a normally non-painful stimulus, e.g., touch and massage), expansion of the receptive field (pain beyond the area of peripheral nerve supply), prolonged electrophysiological discharge, and an after-stimulus unpleasant quality of pain (e.g., burning, throbbing, numbness)” (Yunus, 2008).»
«These symptoms might be mediated by amplified central sensitivity, but peripheral factors, which have been described in FM and irritable bowel syndrome (IBS), may also play a role (e.g., Price et al., 2009; Staud et al., 2009). »
«Staud has shown that local anesthetic injection into trapezius muscle tender points results in lower levels of thermal hyperalgesia in the forearm, consistent with peripheral nociceptive input as a contributor to central sensitization (Staud et al., 2009).»
«The interaction of nerve mechanics and function has been termed neurodynamics. As an example of the principles of neurodynamics, the median nerve elongates approximately 20% as the upper extremity moves from a position of full wrist and elbow flexion to one of full wrist and elbow extension (Butler, 1991). »
» If that ability to elongate is impaired—due to movement restrictions in tissues adjacent to the median nerve and its branches, or due to swelling or adhesions within the median nerve itself—the result is an increase in mechanical tension within the nerve. This adverse neural tension, also termed neurodynamic dysfunction, is thought to contribute to pain and other symptoms through mechanical sensitization and altered nociceptive signaling, altered proprioception, adverse patterns of muscle recruitment and force of muscle contraction, reduced intra-neural blood flow, and release of inflammatory neuropeptides (Lindquist et al., 1973; Kornberg and McCarthy, 1992;Shacklock, 1995; Slater and Wright, 1995; Balster and Jull, 1997; Van der Heide et al., 2001; Kobayashi et al., 2003; Orlin et al., 2005).»
«It is now well-established that manual stretch of nerves is capable of evoking increased sweating and alterations of blood flow in peripheral tissues, providing evidence of electrophysiologic activity in sympathetic nerve fibers (Lindquist et al., 1973; Kornberg and McCarthy, 1992; Slater and Wright, 1995; Orlin et al., 2005). Conversely, treatment of areas of adverse neural tension (for example in carpal tunnel syndrome, cervico-brachial pain, and osteoarthritis) leads to improved functional outcomes (Rozmaryn et al., 1998; Deyle et al., 2000; Tal-Akabi and Rushton, 2000;Akalin et al., 2002; Allison et al., 2002).»
«The most notable examples of these provocation maneuvers are ankle dorsiflexion, the passive straight leg raise test, the upper limb tension (or neurodynamic) tests, and the seated slump test (Butler, 1991,2000). Test-retest reliability is good for straight leg raise, slump testing, and upper limb neurodynamic testing. (Coppieters et al., 2001;Herrington et al., 2008)»
«Because it is not possible to differentiate completely between adverse neural tension and strain in muscles, fascia, and other soft tissues, we will use the more general term “neuromuscular strain” in this paper. »
«As shown on the left in Figure 1, neuromuscular strains and movement restrictions can develop as a result injuries and activities of daily life (for example, due to soft tissue and peri-neural adhesions around scars, contusions and fractures that reduce range of motion, anatomic abnormalities like scoliosis and kyphosis, overuse injuries, and others).»
«If the neuromuscular strains were not treated, and if the individual adapted to the increased symptom burden with decreased activity, then neural, soft tissue and muscular restrictions would be expected to worsen, leading to greater impairment and greater central sensitization. »
«In our clinical work, we have found that neuromuscular restrictions are common in CFS.»
«We have also noted that many symptoms of CFS can be reproduced by selectively adding neuromuscular strain during the examination (Rowe et al., 2013a,b). »
«Despite the elevation of the leg, which might have been expected to improve venous return to the heart and thereby improve blood flow to the brain, lightheadedness increased, as did visual blurring. Both individuals remained more fatigued than usual for 12–24 h. Thus, supine neuromuscular strain provoked increased fatigue and cognitive disturbance, the two symptoms not adequately explained by the central sensitivity hypothesis thus far.»
«We have observed that open treatment of these movement restrictions using manual therapy is associated with clinical improvement (Rowe et al., 2013a,b).»
«The hypothesis can be tested by evaluating the whether the response to a given neuromuscular strain differs between CFS subjects and controls with regard to immediate and delayed (24-h) symptoms, and with regard to measures of central sensitivity, such as changes in heart rate variability, or changes in pain sensitivity as measured by pressure-pain thresholds. «