Svært spennende studie ang pustens påvirkning på vagusnerven, som bekrefter Breathing System sin Autonome pust, 5 sek inn og 5 sek ut, altså 6 pust i minuttet.
Nevner hvordan en usymmetrisk pust, f.eks. 3 inn og 7 ut, ikke påvirker vagusnerven i særlig stor grad. Og at ujjayi påvirker vagusnerven dårligere enn uanstrengt sakte pust. Ujjiayi pust har andre positivie effekter.
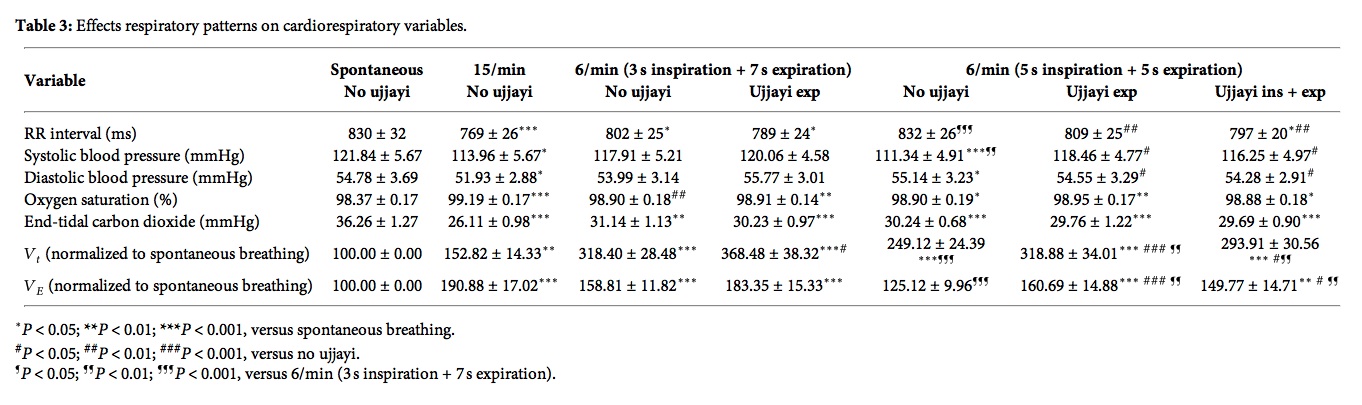
Nevner også at CO2 synker fra 36 til 30 mmHg når man puster 5/5 i forhold til når man ikke gjør pusteteknikk (spontan pust), men synker til 26 mmHg når man puster 15 pust i minuttet. Selv med 7s utpust synker CO2 ned til 31 mmHg. Dette er motsatt av hva studien på CO2 hos angstpasienter viser, hvor CO2 øker selv når pustefrekvensen senkes fra 15 til 12, og øker mer jo saktere pustefrekvensen er.
Nevner også noe svært interessant om at små endinger i oksygenmetning kan gi store endringer oksygentrykket pga bohr-effekt kurven som flater veldig ut ved 98% slik at en 0.5% økning i oksygenmetning kan likevel gir 30% økning i oksygentrykket.
http://www.hindawi.com/journals/ecam/2013/743504/
The slow breathing with equal inspiration and expiration seems the best technique for improving baroreflex sensitivity in yoga-naive subjects. The effects of ujjayi seems dependent on increased intrathoracic pressure that requires greater effort than normal slow breathing.
Respiratory research documents that reduced breathing rate, hovering around 5-6 breaths per minute in the average adult, can increase vagal activation leading to reduction in sympathetic activation, increased cardiac-vagal baroreflex sensitivity (BRS), and increased parasympathetic activation all of which correlated with mental and physical health [1–4]. BRS is a measure of the heart’s capacity to efficiently alter and regulate blood pressure in accordance with the requirements of a given situation. A high degree of BRS is thus a good marker of cardiac health [5].
The slow breathing-induced increase in BRS could be due to the increased tidal volume that stimulates the Hering-Breuer reflex, an inhibitory reflex triggered by stretch receptors in the lungs that feed to the vagus [6]. In addition, the slow breathing increases the oxygen absorption that follows greater tidal volume , as a result of reduction in the effects of anatomical and physiological dead space [7, 8]. This might in turn produce another positive effect, that is, a reduction in the need of breathing. Indeed, a reduction in chemoreflex sensitivity and, via their reciprocal relationships, an increase in BRS, have been documented with slow breathing [9–13].

In comparison to spontaneous breathing, fast breathing led to a reduction in BRS, whilst all slow breathing (with or without ujjayi breathing) increased BRS. This increase was seen in both the symmetrical (5 second inspiration and expiration) and asymmetrical (3 second inspiration and 7 second expiration) slow breathing conditions. Engaging ujjayi breathing on the exhalation had the effect of reducing the increase in BRS of slow breathing alone, and this was further reduced with ujjayi on the inspiration and expiration (which was not significantly higher than baseline). These differences were even more pronounced with respect to controlled breathing at 15 breath/minute, which also showed highly significant differences with respect to spontaneous breathing, but in the opposite direction.
When slow breathing was done in conjunction with ujjayi breathing, oxygen saturation further increased, though only slightly. Overall, however, this was a highly significant change given that baseline oxygen saturation was already high approximately 98.3% (Table
3).
However, with 15 breath/minute controlled breathing the increase in oxygen saturation occurred with a large relative increase in Ve and a marked drop in end-tidal carbon dioxide. Conversely, with slow breathing, the increase in oxygen saturation occurred with only a moderate increase in Ve and drop in carbon dioxide.
The greatest improvement was found in slow breathing without ujjayi, while breathing controlled at a rate of 15/min caused a drop in BRS. In all forms of slow breathing there was a statistically significant increase in oxygen saturation from the mean baseline of 98.3%, confirming the relationship between high levels of oxygen absorption and BRS.
In this study, we show that slow breathing and increased oxygen absorption lead to enhanced BRS. This might result from several possible factors, all interrelated. In theory, the increase in arterial oxygen partial pressure increases blood pressure, which in turn could stimulate the baroreceptors and improve the BRS gain. This was recently observed in healthy [
28] and diabetic subjects [
25]. The seemingly small extent of the increase in oxygen saturation should not be overlooked.
In fact, the haemoglobin dissociation curves states that at higher saturation values small changes reflex large changes in the partial pressure of oxygen.Because the oxygen tension (and not oxygen saturation) is the chemoreflex input signal, this explains why in a previous study the administration of oxygen in normoxia induced a significant increase in BRS and parasympathetic activity despite a small increase in oxygen saturation [
25].
We did not find any significant difference between asymmetrical and symmetrical breathing during slow breathing. We suggest that most of these results could be due to the prolonged expiratory time (in fact the 3-second inspiratory time of the asymmetrical breathing was very close to the spontaneous breathing). In the yoga tradition several degrees of asymmetries were adopted. While some of these could have specific effects (and could be matter for further investigations), our results suggest that an expiratory time of at least 5 seconds was sufficient to elicit most of the results observed.
Based on our findings, slow breathing with similar inspiration and expiration times appears the most effective and simple way to heighten the BRS and improve oxygenation in normoxia. Ujjayi breath demonstrates limited added benefit over slow breathing done at 6/min in normoxia; however, the effects could be more pronounced in hypoxia, and this could be matter for future investigations.