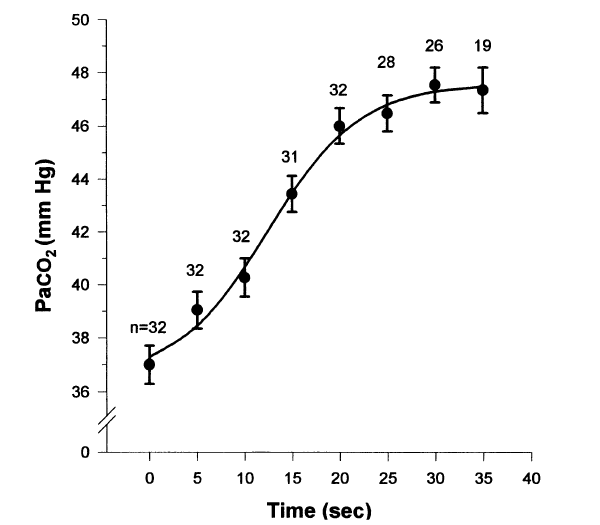
Denne viser hvordan økt CO2 øker oksygenering og blodsirkulasjon i huden og i vevet. Studien er gjort på individer i narkose og med assistert pust med konstant volum på 10ml/kg og pustefrekvens mellom 11 og 14.
Background: Wound infections are common, serious, surgical complications. Oxidative killing by neutrophils is the primary defense against surgical pathogens and increasing intraoperative tissue oxygen tension markedly reduces the risk of such infections. Since hypercapnia improves cardiac output and peripheral tissue perfusion, we tested the hypothesis that peripheral tissue oxygenation increases as a function of arterial carbon dioxide tension (Paco2) in anesthetized humans.
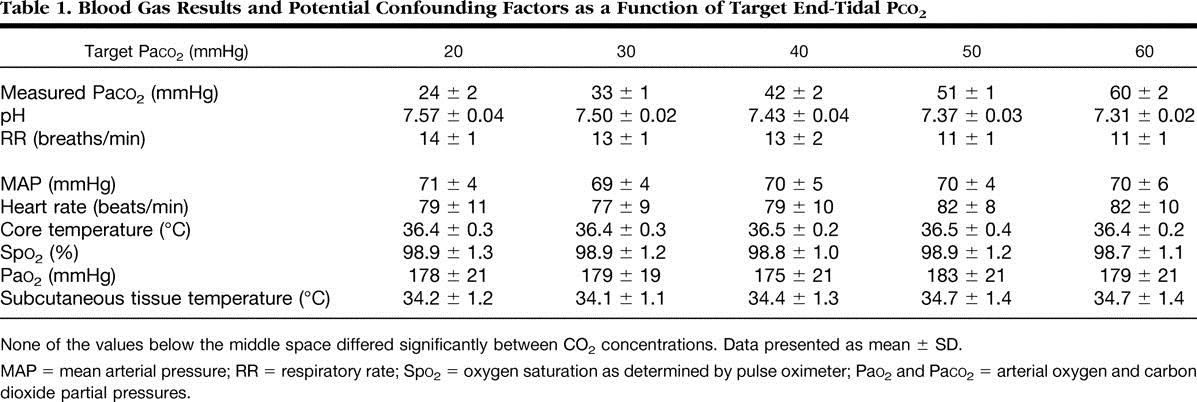
Methods: General anesthesia was induced with propofol and maintained with sevoflurane in 30% oxygen in 10 healthy volunteers. Subcutaneous tissue oxygen tension (Psqo2) was recorded from a subcutaneous tonometer. An oximeter probe on the upper arm measured muscle oxygen saturation. Cardiac output was monitored noninvasively. Paco2 was adjusted to 20, 30, 40, 50, or 60 mmHg in random order with each concentration being maintained for 45 min.
Results: Increasing Paco2 linearly increased cardiac index and Psqo2: Psqo2 = 35.42 + 0.77 (Paco2), P < 0.001.
Conclusions: The observed difference in PsqO2 is clinically important because previous work suggests that comparable increases in tissue oxygenation reduced the risk of surgical infection from −8% to 2 to 3%. We conclude that mild intraoperative hypercapnia increased peripheral tissue oxygenation in healthy human subjects, which may improve resistance to surgical wound infections.

This hypercapnia-induced increase in cardiac output results in higher tissue oxygen pressure. In the current study Psqo2 went from 58 to 74 mmHg with only a 20-mmHg increase in Paco2. This increase in Psqo2 is likely to be clinically important because it is associated with a substantial reduction in the risk of surgical wound infection. 11 These results suggest that maintaining slight hypercapnia is likely to reduce the risk of surgical wound infection. Carbon dioxide management thus joins the growing list of anesthetic factors that do or are likely to influence the risk of wound infection.
Hypercapnia appears to provide other benefits as well. 35 For example, hypercapnia and hypercapnic acidosis decrease ischemia–reperfusion injury by inhibiting xanthine oxidase in an in vitro model of acute lung injury. 36 Hypercapnia similarly improves functional recovery and coronary blood flow during hypercapnic acidosis in an isolated blood-perfused heart model. 37 Furthermore, small tidal volume ventilation (associated with mild hypercapnia) and permissive hypercapnia have been shown to improve the outcome of patients with acute respiratory distress syndrome as a result of decreased mechanical stretch of the diseased pulmonary tissues. 38,39
Hypercapnia also increases cerebral blood flow and decreases cerebrovascular resistance through dilation of arterioles whereas hypocapnia does the opposite. 40,41 In a recent study, hyper- and hypocapnia were shown to influence brain oxygen tension in swine during hemorrhagic shock 42; hyperventilation and the resulting hypocapnia (15–20 mmHg) decreased cerebral oxygen pressure a further 56%. Hypercapnia has been utilized clinically to improve cerebral perfusion during carotid endarterectomy 43,44 and for emergency treatment of retinal artery occlusion. 45