Artikkel som oppsummer gluten-problemet, fra Dr. Mark Hyman.
Kategoriarkiv: Forskning og artikler
This Coach Improved Every Tiny Thing by 1 Percent and Here’s What Happened
Success is a few simple disciplines, practiced every day; while failure is simply a few errors in judgment, repeated every day.
—Jim Rohn
Artikkelen beskriver verdien i «aggregation of marginal gains.», den samlede effekten av 1% økning i mange områder av livet gir bedre resltater enn stør økning i få områder. Nevner eksempel med et Tour De France team.
This Coach Improved Every Tiny Thing by 1 Percent and Here’s What Happened
Uncertainty Increases Pain: Evidence for a Novel Mechanism of Pain Modulation Involving the Periaqueductal Gray
Om at følelsen av usikkerhet gir økt smerte.
http://www.jneurosci.org/content/33/13/5638.full
Predictions about sensory input exert a dominant effect on what we perceive, and this is particularly true for the experience of pain. However, it remains unclear what component of prediction, from an information-theoretic perspective, controls this effect. We used a vicarious pain observation paradigm to study how the underlying statistics of predictive information modulate experience. Subjects observed judgments that a group of people made to a painful thermal stimulus, before receiving the same stimulus themselves. We show that the mean observed rating exerted a strong assimilative effect on subjective pain. In addition, we show that observed uncertainty had a specific and potent hyperalgesic effect. Using computational functional magnetic resonance imaging, we found that this effect correlated with activity in the periaqueductal gray. Our results provide evidence for a novel form of cognitive hyperalgesia relating to perceptual uncertainty, induced here by vicarious observation, with control mediated by the brainstem pain modulatory system.
Cc to the brain: how neurons control fine motor behavior of the arm
OM at ryggraden utviklet seg før hjernen, og at det viser seg at ryggraden sender signaler ikke bare ut i armer og bein, men samtidig opp til hjernen.
http://www.unibas.ch/index.cfm?uuid=E34D435E99D6097F77CE8C5E0D49B1B2&type=search&show_long=1
Chiara Pivetta, first author of the publication, explains: “The motor command to the muscle is sent in two different directions – in one direction, to trigger the desired muscular contraction and in the other, to inform the brain that the command has actually been passed on to the musculature.” In analogy to e mail transmission, the information is thus not only sent to the recipient but also to the original requester.
Interestingly, the scientists only observed this kind of information flow to the brain for arm, but not for leg control. “What this shows,” says Arber, “is that this information pathway is most likely important for fine motor skills. Compared to the leg, movements of our arm and especially our hands have to be far more precise. Evidently, our body can only ensure this level of accuracy in motor control with constant feedback of information.”
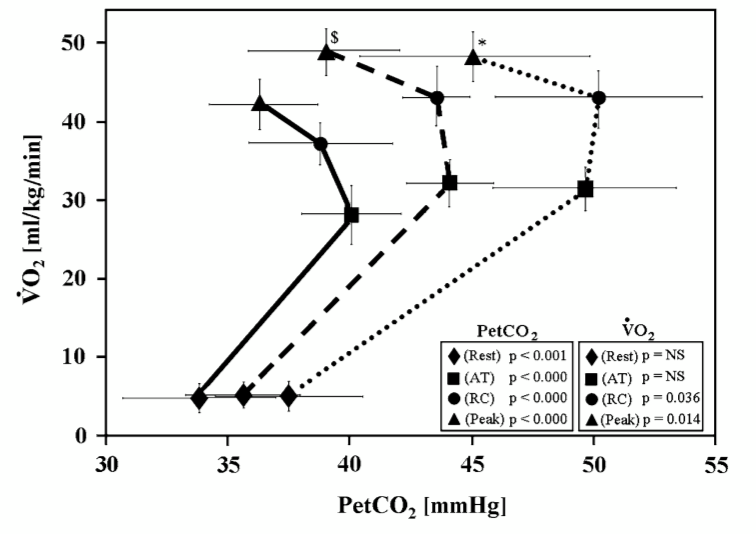
End-tidal pressure of CO2 and exercise performance in healthy subjects.
høyere melkesyreterskel med høyere co2: http://www.ncbi.nlm.nih.gov/pubmed/18521623/
Klikk for å få tilgang til PUBBL%2034_2.pdf
Måle Vitalkapasitet (lungevolum) med ballong
Denne videoen beskriver hvordan vital kapasitet måles enkelt med en ballong. En greit teknikk å bruke for å sjekke din fremgang med diafragma øvelsene i Verkstedet Breathing System.
Den nevner også hvordan man regner ut kroppens overflateareal, Body Surface Area: BSA = roten av ( (høyde (cm)*vekt (kg)) / 3600)
For så å kunne beregnes hva en vital kapsitet burde være (svaret vises i kubikkcentimeter, cm3):
Menn: BSA * 2500
Kvinner: BSA * 2000
Den virkelige vitalkapsiteten måles ved å blåse i en ballong (som er strekt ut først for å gjøre den mest mulig rund) 3 ganger, og så forholde seg til det største volumet.
Ballong diameteren viser lungevolum i denne grafen:
Man regner med at alt over 80% av forventet vitalkapsitet er normalt.
D vitamin inntak regnet fra kroppsvekt
More specifically, the researchers calculated from their data that a total input of 70-80 IU/day/kg-of-body-weight is needed to achieve 25(OH)D of 40 ng/mL.
http://updates.pain-topics.org/2013/12/is-5000-iuday-of-vitamin-d-enough-for.html?m=1
Ten Steps to Understanding Manual and Movement Therapies for Pain
Alt om smerte, kort fortalt, fra: http://www.somasimple.com/forums/showthread.php?t=4942
Nothing Simple – Ten Steps to Understanding Manual and Movement Therapies for Pain
1. Pain is a category of complex experiences, not a single sensation produced by a single stimulus.
2. Nociception (warning signals from body tissues) is neither necessary nor sufficient to produce pain. In other words, pain can occur in the absence of tissue damage.
3. A pain experience may be induced or amplified by both actual and potential threats.
4. A pain experience may involve a composite of sensory, motor, autonomic, endocrine, immune, cognitive, affective and behavioural components. Context and meaning are paramount in determining the eventual output response.
5. The brain maps peripheral and central neural processing into each of these components at multiple levels. Therapeutic input at a single level may be sufficient to resolve a threat response.
6. Manual and movement therapies may affect peripheral and central neural processes at various stages:
– transduction of nociception at peripheral sensory receptors
– transmission of nociception in the peripheral nervous system
– transmission of nociception in the central nervous system
– processing and modulation in the brain
7. Therapies that are most likely to be successful are those that address unhelpful cognitions and fear concerning the meaning of pain, introduce movement in a non-threatening internal and external context, and/or convince the brain that the threat has been resolved.
8. The corrective physiological mechanisms responsible for resolution are inherent. A therapist need only provide an appropriate environment for their expression.
9. Tissue length, form or symmetry are poor predictors of pain. The forces applied during common manual treatments for pain generally lack the necessary magnitude and specificity to achieve enduring changes in tissue length, form or symmetry. Where such mechanical effects are possible, the clinical relevance to pain is yet to be established. The predominant effects of manual therapy may be more plausibly regarded as the result of reflexive neurophysiological responses.
10. Conditioning for the purposes of fitness and function or to promote general circulation or exercise-induced analgesia can be performed concurrently but points 6 and 9 above should remain salient.
Bibliography
Books:
Pain: The Science of Suffering – Patrick Wall
The Challenge of Pain – Patrick Wall, Ronald Melzack
Explain Pain – David Butler, Lorimer Moseley
The Sensitive Nervous System – David Butler
Phantoms in the Brain – V. S. Ramachandran
Topical Issues in Pain Vol’s 1-5 – Louis Giffiord (ed)
The Feeling of What Happens – Antonio Damasio
Clinical Neurodynamics – Michael Shacklock
Eyal Lederman – The Science and Practice of Manual Therapy
Research articles:
Melzack R. Pain and the neuromatrix in the brain. J Dental Ed. 2001;65:1378-82.
Craig AD. Pain mechanisms: Labeled lines versus convergence in central processing. Ann Rev Neurosci. 2003;26:130.
Craig AD. How do you feel? Interoception: the sense of the physiological condition of the body. Nature Rev Neurosci. 2002;3:655-66.
Henderson LA, Gandevia SC, Macefield VG. Somatotopic organization of the processing of muscle and cutaneous pain in the left and right insula cortex: A single-trial fMRI study. Pain. 2007;128:20-30.
Olausson H, Lamarre Y, Backlund H, Morin C, Wallin BG, Starck G, Ekholm S, Strigo I, Worsley K, Vallbo AB, Bushnell MC. Unmyelinated tactile afferents signal touch and project to insular cortex. Nature Neurosci. 2002;5:900–904.
Moseley GL. A pain neuromatrix approach to patients with chronic pain. Manual Ther. 2003;8:130-40.
Moseley GL. Unravelling the barriers to reconceptualisation of the problem in chronic pain: The actual and perceived ability of patients and health professionals to understand the neurophysiology. J Pain. 2003;4:184-89.
Moseley GL, Arntz A. The context of a noxious stimulus affects the pain it evokes. Pain. 2007;133(1-3):64-71.
Moseley, GL, Nicholas, MK and Hodges, PW. A randomized controlled trial of intensive neurophysiology education in chronic low back pain. Clin J Pain. 2004;20:324-30.
Crombez G, Vlaeyen JWS, Heuts PH et al. Pain-related fear is more disabling than pain itself. Evidence on the role of pain-related fear in chronic back pain disability. Pain. 1999;80:329-40.
Zusman M. Forebrain-mediated sensitization of central pain pathways: ‘non-specific’ pain and a new image for manual therapy. Manual Ther. 2002;7:80-88.
Dorko B. The analgesia of movement: Ideomotor activity and manual care. J Osteopathic Med. 2003;6:93-95.
Threlkeld AJ. The effects of manual therapy on connective tissue. Phys Ther. 1992;72:893-902.
Lederman E. The myth of core stability. Retrieved at: http://www.ppaonline.co.uk/
Brains are foretelling devices
«brains are foretelling devices and their predictive powers emerge from the various rhythms they perpetually generate. At the same time, brain activity can be tuned to become an ideal observer of the environment, due to an organized system of rhythms.» —Gyorgy Buzsaki, author of Rythms of the Brain
A meta-ethnography of patients’ experience of chronic non-malignant musculoskeletal pain
Omfattende studie om kronisk smerte som kommer med reelle tiltak for å bedre tilstanden hos pasientene. Nevner spesielt en at en holdningsendring må skje hos legene og sykepleierene hvor man inkluderer pasientes subjektive opplevelse. Nevner grunnlaget for dagens medisin og objektifisering av pasienten: «Foucault412 described the paradoxical position of the clinical encounter, in which the doctor aims to diagnose a disease rather than understand the person’s experience: ‘If one wishes to know the illness from which he is suffering, one must subtract the individual, with his [or her] particular qualities’ »
http://www.journalslibrary.nihr.ac.uk/__data/assets/pdf_file/0010/94285/FullReport-hsdr01120.pdf
Conclusion: Our model helps us to understand the experience of people with chronic MSK pain as a constant adversarial struggle. This may distinguish it from other types of pain. This study opens up possibilities for therapies that aim to help a person to move forward alongside pain. Our findings call on us to challenge some of the cultural notions about illness, in particular the expectation of achieving a diagnosis and cure. Cultural expectations are deep-rooted and can deeply affect the experience of pain. We therefore should incorporate cultural categories into our understanding of pain. Not feeling believed can have an impact on a person’s participation in everyday life. The qualitative studies in this meta-ethnography revealed that people with chronic MSK pain still do not feel believed. This has clear implications for clinical practice. Our model suggests that central to the relationship between patient and practitioner is the recognition of the patient as a person whose life has been deeply changed by pain. Listening to a person’s narratives can help us to understand the impact of pain. Our model suggests that feeling valued is not simply an adjunct to the therapy, but central to it. Further conceptual syntheses would help us make qualitative research accessible to a wider relevant audience. Further primary qualitative research focusing on reconciling acceptance with moving forward with pain might help us to further understand the experience of pain. Our study highlights the need for research to explore educational strategies aimed at improving patients’ and clinicians’ experience of care.
As part of a person’s struggle we described the fragmentation of body and self, and suggested that moving forward with pain involves a process of reintegrating the painful body.
Under conditions of health, we perform actions automatically and remain unaware of our body until something goes wrong with it. Health presupposes that we remain unaware of our bodies.396 When in pain, the body emerges as an ‘alien presence’;
it ‘dys-appears’. I no longer am a body but have a body,388 and my body becomes an ‘it’ as opposed to an
I’. Wall399 describes this dualism as epitomised by the expression ‘my foot hurts me’ as if in some way the foot is apart from myself (p. 23). It is because ‘the body seizes our awareness particularly at times of disturbance, [that] it can come to appear “other” and opposed to the self’ (p. 70).388 This fragmentation of ‘mind trapped inside an alien body’ means that our bodies become mistrusted and ‘forgotten as a ground of knowledge’ (p. 86).388 Our concept ‘integrating my painful body’ implies an altered therapeutic relationship with the body in which the dualism of mind and body are broken down.
We do not know why certain patients can accept and redefine their sense of self and others cannot.
It may be related to the degree of disruption to self that is caused by pain. The enmeshment model developed by Pincus and Morley406 proposes that, if a person regards their ideal self as unobtainable in the presence of pain, they are less likely to accept chronic pain. The enmeshment model incorporates self-discrepancy theory,407 which proposes that the extent to which pain disrupts our lives depends on the meaning that it holds for us. In self-discrepancy theory meaning incorporates three constructs: (1) actual self – ‘your representation of the attributes that someone (yourself or another) believes you actually possess’; (2) ideal self – ‘your representation of the attributes that someone (yourself or another) would like you, ideally, to possess’; and (3) ought self – ‘your representation of the attributes that someone (yourself or another) believes you should or ought to possess’ (p. 320–1).407
However, it is ‘pathos’, the feeling of suffering and powerlessness, of ‘life going wrong’, that precedes a person’s visit to the doctor (p. 137).396 Our model suggests that central to the therapeutic relationship is the recognition of ‘pathos’; the patient is a subject rather than an ‘object’ of investigation. This concept is central to models of patient-centred care.413
We described a need for a person in pain to feel that the health-care professional is alongside them with their pain. Affirming a person’s experience and allowing an empathetic interpretation of their story is not an adjunct, but integral to health care.395
Our model also suggests possibilities that might help patients to move forward alongside their pain:
- an integrated relationship with the painful body
- redefining a positive sense of self now and in the future
- communicating to, rather than hiding from, others the experience of pain
- knowing that I am not the only one with pain (but I am still valued)
- regaining a sense of reciprocity and social participation
- recognising the limitations of the medical model
- being empowered to experiment and change the way that I do things without the sanction of the health-care professional.
