Pdf foredrag om alle faktorer som styrer pustefrekvensen.
Klikk for å få tilgang til Lec%208%202013%20Control%20of%20Breathing.pdf
Pdf foredrag om alle faktorer som styrer pustefrekvensen.
Klikk for å få tilgang til Lec%208%202013%20Control%20of%20Breathing.pdf
Alt om smerte, kort fortalt, fra: http://www.somasimple.com/forums/showthread.php?t=4942
Nothing Simple – Ten Steps to Understanding Manual and Movement Therapies for Pain
1. Pain is a category of complex experiences, not a single sensation produced by a single stimulus.
2. Nociception (warning signals from body tissues) is neither necessary nor sufficient to produce pain. In other words, pain can occur in the absence of tissue damage.
3. A pain experience may be induced or amplified by both actual and potential threats.
4. A pain experience may involve a composite of sensory, motor, autonomic, endocrine, immune, cognitive, affective and behavioural components. Context and meaning are paramount in determining the eventual output response.
5. The brain maps peripheral and central neural processing into each of these components at multiple levels. Therapeutic input at a single level may be sufficient to resolve a threat response.
6. Manual and movement therapies may affect peripheral and central neural processes at various stages:
– transduction of nociception at peripheral sensory receptors
– transmission of nociception in the peripheral nervous system
– transmission of nociception in the central nervous system
– processing and modulation in the brain
7. Therapies that are most likely to be successful are those that address unhelpful cognitions and fear concerning the meaning of pain, introduce movement in a non-threatening internal and external context, and/or convince the brain that the threat has been resolved.
8. The corrective physiological mechanisms responsible for resolution are inherent. A therapist need only provide an appropriate environment for their expression.
9. Tissue length, form or symmetry are poor predictors of pain. The forces applied during common manual treatments for pain generally lack the necessary magnitude and specificity to achieve enduring changes in tissue length, form or symmetry. Where such mechanical effects are possible, the clinical relevance to pain is yet to be established. The predominant effects of manual therapy may be more plausibly regarded as the result of reflexive neurophysiological responses.
10. Conditioning for the purposes of fitness and function or to promote general circulation or exercise-induced analgesia can be performed concurrently but points 6 and 9 above should remain salient.
Bibliography
Books:
Pain: The Science of Suffering – Patrick Wall
The Challenge of Pain – Patrick Wall, Ronald Melzack
Explain Pain – David Butler, Lorimer Moseley
The Sensitive Nervous System – David Butler
Phantoms in the Brain – V. S. Ramachandran
Topical Issues in Pain Vol’s 1-5 – Louis Giffiord (ed)
The Feeling of What Happens – Antonio Damasio
Clinical Neurodynamics – Michael Shacklock
Eyal Lederman – The Science and Practice of Manual Therapy
Research articles:
Melzack R. Pain and the neuromatrix in the brain. J Dental Ed. 2001;65:1378-82.
Craig AD. Pain mechanisms: Labeled lines versus convergence in central processing. Ann Rev Neurosci. 2003;26:130.
Craig AD. How do you feel? Interoception: the sense of the physiological condition of the body. Nature Rev Neurosci. 2002;3:655-66.
Henderson LA, Gandevia SC, Macefield VG. Somatotopic organization of the processing of muscle and cutaneous pain in the left and right insula cortex: A single-trial fMRI study. Pain. 2007;128:20-30.
Olausson H, Lamarre Y, Backlund H, Morin C, Wallin BG, Starck G, Ekholm S, Strigo I, Worsley K, Vallbo AB, Bushnell MC. Unmyelinated tactile afferents signal touch and project to insular cortex. Nature Neurosci. 2002;5:900–904.
Moseley GL. A pain neuromatrix approach to patients with chronic pain. Manual Ther. 2003;8:130-40.
Moseley GL. Unravelling the barriers to reconceptualisation of the problem in chronic pain: The actual and perceived ability of patients and health professionals to understand the neurophysiology. J Pain. 2003;4:184-89.
Moseley GL, Arntz A. The context of a noxious stimulus affects the pain it evokes. Pain. 2007;133(1-3):64-71.
Moseley, GL, Nicholas, MK and Hodges, PW. A randomized controlled trial of intensive neurophysiology education in chronic low back pain. Clin J Pain. 2004;20:324-30.
Crombez G, Vlaeyen JWS, Heuts PH et al. Pain-related fear is more disabling than pain itself. Evidence on the role of pain-related fear in chronic back pain disability. Pain. 1999;80:329-40.
Zusman M. Forebrain-mediated sensitization of central pain pathways: ‘non-specific’ pain and a new image for manual therapy. Manual Ther. 2002;7:80-88.
Dorko B. The analgesia of movement: Ideomotor activity and manual care. J Osteopathic Med. 2003;6:93-95.
Threlkeld AJ. The effects of manual therapy on connective tissue. Phys Ther. 1992;72:893-902.
Lederman E. The myth of core stability. Retrieved at: http://www.ppaonline.co.uk/
Dette klippet nevner forskningen til den svenske nevrokirurgen Alfred Breig og viser til at det er hofteleddet som bestemmer det meste i nervesystemets tensjon (strekk). Utoverrotasjon og lett abduksjon gir minst strekk i nervesystemet.
«Tension in the nervous system has the same effect as compression» – Barret Dorko
En review studie fra 2012 som inneholder det meste om Magnesium, spesielt rettet mot betennelser i hjerte/kar og nervesystemet.
http://www.karger.com/Article/FullText/339380
Magnesium L-lactate and L-aspartate are the oral magnesium compounds that have the greatest bioavailability, are the most water-soluble and have the greatest serum and plasma concentrations [8].
After a mean follow-up of 9.8 years and adjusting for confounders, the authors concluded that women in the highest quintile (an intake of 400 mg/day of magnesium) had a decreased HTN (hypertension) risk (p < 0.0001) versus those in the lowest quintile (approx. 200 mg/day of magnesium) [20].
Because of magnesium’s anti-inflammatory, statin-like and anti-mineralizing effects, a role for it is emerging in cardiovascular and neurological medicine.
The potential impact of magnesium in cardiovascular and neurological health, the abundance and low cost of the supplement, the relatively low side effect profile and the paucity of information in the literature about this common mineral suggest that more studies should be conducted to determine its safety and efficacy. The majority of human trials with magnesium thus far have not been interventional, but based on food questionnaires which may not be accurate and are subject to a recall bias. Further work is also needed to determine the mechanism of action by which magnesium modulates the mineralization and inflammation of the cardiovascular and nervous systems.
Magnesium gjør at nervesystemet blir mindre sensitivt i studie på rotter med nevropati. Dosen er beregnet til å være ca 147 mg pr dag (24t), som er veldig mye relativt til kroppsvekten på en mus på 10-20g. Om vi regner det om til menneskevekt blir det megadoser.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3002451/
Neuropathic pain is a common diabetic complication affecting 8–16% of diabetic patients. It is characterized by aberrant symptoms of spontaneous and stimulus-evoked pain including hyperalgesia and allodynia. Magnesium (Mg) deficiency has been proposed as a factor in the pathogenesis of diabetes-related complications, including neuropathy. In the central nervous system, Mg is also a voltage-dependant blocker of the N-methyl-d-aspartate receptor channels involved in abnormal processing of sensory information. We hypothesized that Mg deficiency might contribute to the development of neuropathic pain and the worsening of clinical and biological signs of diabetes and consequently, that Mg administration could prevent or improve its complications. We examined the effects of oral Mg supplementation (296 mg l−1 in drinking water for 3 weeks) on the development of neuropathic pain and on biological and clinical parameters of diabetes in streptozocin (STZ)-induced diabetic rats. STZ administration induced typical symptoms of type 1 diabetes. The diabetic rats also displayed mechanical hypersensitivity and tactile and thermal allodynia. The level of phosphorylated NMDA receptor NR1 subunit (pNR1) was higher in the spinal dorsal horn of diabetic hyperalgesic/allodynic rats. Magnesium supplementation failed to reduce hyperglycaemia, polyphagia and hypermagnesiuria, or to restore intracellular Mg levels and body growth, but increased insulinaemia and reduced polydipsia. Moreover, it abolished thermal and tactile allodynia, delayed the development of mechanical hypersensitivity, and prevented the increase in spinal cord dorsal horn pNR1. Thus, neuropathic pain symptoms can be attenuated by targeting the Mg-mediated blockade of NMDA receptors, offering new therapeutic opportunities for the management of chronic neuropathic pain.
Diabetes is also the most common pathological state in which secondary magnesium (Mg) deficiency occurs. Indeed, Mg deficiency has been described in 25–30% and 13.5–47.7% of type 1 and type 2 diabetic patients, respectively (Garland, 1992; Tossielo, 1996; Corsonelloet al. 2000; Engelen et al. 2000; Rodriguez-Moran & Guerrero-Romero, 2003; Pham et al.2007) and its incidence is correlated to diabetes complications (De Leeuw, 2001). Mg is an ATPase allosteric effector involved in inositol transport (Grafton et al. 1992) and the impaired Na+/K+-ATPase activity in peripheral nerves of diabetic animals (Garland, 1992) plays a role in the pathophysiology of diabetic neuropathy (Li et al. 2005).
In the central nervous system, Mg has voltage-dependent blocking properties that play an important role in pain processing at the N-methyl-d-aspartate (NMDA) receptor channel complex (Mayer et al. 1984; Xiao & Bennett, 1994; Begon et al. 2000). In vitro, this blockade operates at extracellular Mg concentrations of less than 1 mm (Mayer et al. 1984), i.e. within the ranges found in human and animal cerebrospinal fluid and plasma (Morris, 1992). The excess release of glutamate from central nociceptor terminals due to nerve damage releases Mg blockade and activates NMDA receptors known to trigger painful sensations (hyperalgesia, allodynia) and alter the sensitivity of postsynaptic cells, resulting in central sensitization (Bennett, 2000). This central sensitization involving the NMDA receptor can be induced in rats in vivo by Mg depletion (Alloui et al. 2003). Several studies suggest that phosphorylation of the NMDA receptor NR1 subunit is correlated to the presence of signs of neuropathy and to persistent pain following nerve injury (Gao et al.2005; Ultenius et al. 2006; Gao et al. 2007; Roh et al. 2008).
One week after STZ or distilled water injection, the animals were assigned to the following three experimental groups:

Water intake was 10-fold and sixfold higher in non-supplemented and MgSO4-supplemented STZ-D rats, respectively, compared with non-diabetic rats. Water intake was significantly lower in MgSO4-supplemented STZ-D rats than non-supplemented STZ-D rats (Table 1). Consequently, urine excretion was 24-fold higher in non-supplemented STZ-D rats than non-diabetic rats. The MgSO4-supplemented STZ-D rats also developed polyuria corresponding to a 15-fold increase in urine excretion compared with non-diabetic rats, but which was nevertheless lower than the increase in non-supplemented STZ-D rats (Table 1). Polyuria in STZ-D rats was significantly correlated to water intake (P < 0.001).
| Parameter | Non-diabetic | Non-suppl. STZ-D | MgSO4-suppl. STZ-D |
|---|---|---|---|
| Water intake (ml (24 h)−1) | 35.22 ± 2.36 | 376.6 ± 32.87*** | 214.4 ± 30.87***,### |
| Urine excretion (ml (24 h)−1) | 12.45 ± 1.51 | 300.1 ± 24.16*** | 184.4 ± 25.23***,## |
| Food intake (g (24 h)−1) | 30.7 ± 1.83 | 54.66 ± 3.67** | 42.06 ± 6.21 |
| Total Mg intake (mg (24 h)−1) | 61.40 ± 3.66 | 109.32 ± 7.34*** | 147.58 ± 1.58***,### |

Figure 4: Time course of mechanical sensitivity measured by paw pressure-induced vocalization threshold (VT) variations in non-diabetic (Non-D), non-supplemented STZ-diabetic (Non-suppl. STZ-D) and MgSO4-supplemented (MgSO4-suppl. STZ-D) rats
| Parameter | Non-diabetic | Non-suppl. STZ-D | MgSO4-suppl. STZ-D |
|---|---|---|---|
| Tactile hypersensitivity | |||
| Week 2 | 0/10 | 3/10 | 0/10# |
| Week 4 | 0/10 | 6/10* | 0/10# |
| Thermal hypersensitivity | |||
| Week 2 | 0/10 | 6/10* | 0/10# |
| Week 4 | 0/10 | 6/10* | 0/10# |
This study clearly showed that Mg supplementation prevents tactile and thermal allodynia and attenuates and delays mechanical hyperalgesia in STZ-D rats. This effect was mediated, at least in part, by the prevention of NMDA receptor NR1 subunit phosphorylation in STZ-D rats. However, the study also showed that Mg supplementation did not improve most of the biological and clinical signs of diabetes despite restoration of normal insulin secretion.
Omfattende gjennomgang om hvordan nevrogene betennelser fungerer fysiologisk. Nevner at betennelser ikke er problemet, men en funksjon kroppen benytter seg av for å håndtere problemer som giftstoffer og metabolsk problemer. Derfor nytter det ikke å dempe betennelsen. Man MÅ fjerne årsaken til betennelsen…
http://www.ncbi.nlm.nih.gov/pubmed/24281245
http://www.nature.com/nrn/journal/vaop/ncurrent/full/nrn3617.html
The CNS is endowed with an elaborated response repertoire termed ‘neuroinflammation’, which enables it to cope with pathogens, toxins, traumata and degeneration. On the basis of recent publications, we deduce that orchestrated actions of immune cells, vascular cells and neurons that constitute neuroinflammation are not only provoked by pathological conditions but can also be induced by increased neuronal activity. We suggest that the technical term ‘neurogenic neuroinflammation’ should be used for inflammatory reactions in the CNS in response to neuronal activity. We believe that neurogenic neuro-inflammation maintains homeostasis to enable the CNS to cope with enhanced metabolic demands and increases the computational power and plasticity of CNS neuronal networks. However, neurogenic neuroinflammation may also become maladaptive and aggravate the outcomes of pain, stress and epilepsy.



Denen Studien beskriver Stephen Porges sitt arbeid med å forstå Vagus nerven og hvordan den forholder seg til pusten og til psyken.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1868418/
The Polyvagal Theory introduced a new perspective relating autonomic function to behavior that included an appreciation of autonomic nervous system as a “system,” the identification of neural circuits involved in the regulation of autonomic state, and an interpretation of autonomic reactivity as adaptive within the context of the phylogeny of the vertebrate autonomic nervous system. The paper has two objectives: First, to provide an explicit statement of the theory; and second, to introduce the features of a polyvagal perspective. The polyvagal perspective emphasizes how an understanding of neurophysiological mechanisms and phylogenetic shifts in neural regulation, leads to different questions, paradigms, explanations, and conclusions regarding autonomic function in biobehavioral processes than peripheral models. Foremost, the polyvagal perspective emphasizes the importance of phylogenetic changes in the neural structures regulating the autonomic nervous system and how these phylogenetic shifts provide insights into the adaptive function and the neural regulation of the two vagal systems
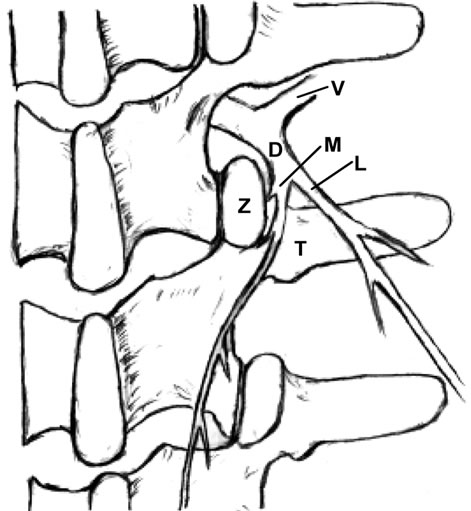
Om hudnære nerver sin rolle i korsryggsmerter. Beskriver spesielt nervene ved L1-2 som går ned til huden i korsryggen og hoftene. Nevner flere interessante diagnosekriterier. Men som de legene og kirurgene forskerne er, har de kun nerveblokkade og kirurgi i som behandlingmuligheter, fullstendig ignorante til mulighetene i manuell behandling. Selv nerveblokkade har 85% av pasientene får mer enn 50% bedring i symptomene, ikke så annerledes enn hva vi forventer med manuell behandling og en intelligent tilnærming til nervesystemet.
Each spinal dorsal ramus arises from the spinal nerve and then divides into a medial and lateral branch. The medial branch supplies the tissues from the midline to the zygapophysial joint line and innervates two to three adjacent zygapophysial joints and their related soft tissues. The lateral branch innervates the tissues lateral to the zygapophysial joint line.
Clinically, L1 and L2 are the most common sites of dorsal rami involvement.
The etiologies of low back pain are numerous. Anatomically, lumbar muscle strain [1,2], lumbar zygapophysial joint syndrome [3-11], instability of the lumbar spine [12], discogenic back pain [1,13], and sacroiliac joint syndrome [2] can cause low back pain. Mechanical pressure on the nerve roots, which may interfere with venous return of the nerve root [14], epidural fibrosis [15], perineural and intraneural fibrosis [16], are additional factors to consider. Additionally, some authors have suggested that the iliolumbar ligament inserting on the lumbar spine is a source of back pain [17].
Anatomically, Bogduk’s work exposed the medial branches of the lumbar spinal dorsal rami as a potential player in low back pain [23-25]. Sihvonen et al. blocked the medial dorsal ramus branch, which resulted in relief of muscle spasms and they suggested that this treatment would aid in improving lumbopelvic rhythm and reducing low back pain [26-29]. These studies supported spinal dorsal ramus as a potential pain generator.
http://file.scirp.org/Html/9-2400120/b3c5afd3-5aa8-4350-9ecc-22fe3e3cc027.jpg
http://file.scirp.org/Html/9-2400120/c6242d6a-bc68-420a-bd92-3c9e7fbafa2d.jpg
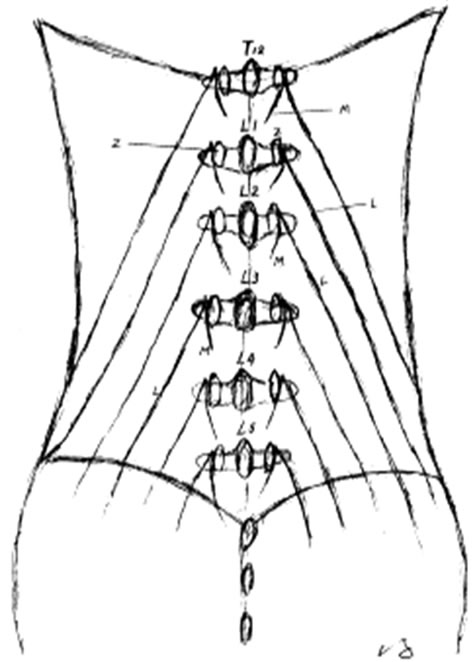
The distribution area of each dorsal ramus is characterized by an overlapping multiple segmental innervations, e.g., the L4 zygapophysial joint is innervated by the L3 and L4 medial branches. Therefore, if single dorsal ramus is irritated proximally, a patient could experience pain at the distal site of this nerve distribution (referred pain). This phenomenon mimics radicular pain, for example, a patient with L4-5 herniated disc experiences pain on his dorsal foot. Thus, a local anesthetic injected to the referred pain area will not relieve pain, because the pain is caused by irritation at the proximal dorsal ramus (see below) [36].
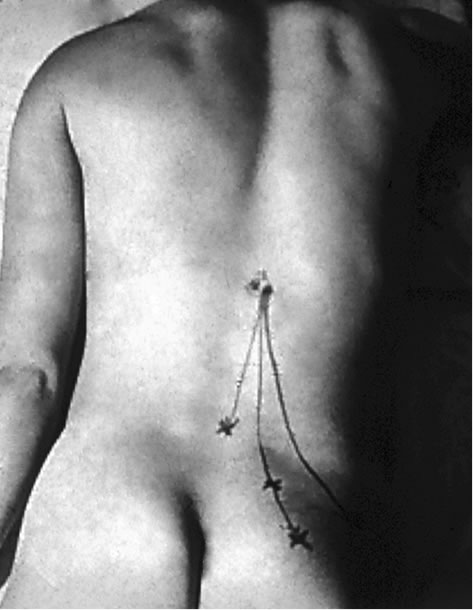
In patients with the spinal dorsal ramus mediated pain, their symptoms usually are on one side and are exacerbated by lumbar extension and/or rotation. This pain may radiate to the ipsilateral low back and buttock region (referred pain) [21,22] (Figure 2). Some patients may present paraspinal muscle spasm (Figure 3(a)). Hyperesthesia may present in the affected dermatome [10,21,22,31,35, 45,46].
http://file.scirp.org/Html/9-2400120/e412d7c3-e859-4500-b82d-396e71f6b638.jpg
The zygapophysial joint line demarcates the distribution of the medial and lateral branches. Pain at between the midline and the zygapophysial joint line or the paraspinal sacroiliac region is caused by on irritated medial branch. Pain lateral to the zygapophysial joint line with radiation to the lateral iliac crest is induced by the lateral branch involvement [19,22]. When the common dorsal ramus is involved, pain will be at the territories of both medial and lateral branches [36,38,47] (Figure 2).
There are some clinical findings in the patient with the spinal dorsal ramus mediated low back pain. The patient usually points to pain at the distal low back (referred pain) [19,22,47]. When the patient bends forward, there is usually a palpable step-off at the affected spinous processes and this is typically two to three segments above the referred pain [47]. There is a palpably widened space and deep tenderness between the spinous processes below the stepoff. With deep palpation of the junction of the same level lateral zygapophysial joint and proximal transverse process, the patient will experience pain and referred pain [19-22,36,47] (Figure 2). Additionally, patients may present an ipsilateral segmental muscle spasm, and a mild scoliosis at the affected vertebral level when the medial branch is involved (Figure 3(a)) [36,47]. If the lateral branch is involved, palpating the longissimus and the iliocostalis muscles can be painful [19-22,35,36,47]. Maigne’s examination techniques are to provoke pain by applying pressure to the lateral aspect of the spinous processes and rubbing the ipislateral facet at the thoracolumbar junction [19-22]. Other findings such as motor, sensory and straight leg raising tests are unremarkable. When the low back pain patient presents pain with radiation below the knee and positive nerve root signs such as loss of sensory or motor function or reflexes in the distribution of the ventral ramus, the ventral ramus involvement (lumbar radiculopathy) should be considered [1].
Any abnormality of the zygapophysial joint such as vertebral malrotation or muscle spasm as well as structural changes of the zygapophysial joint such as subluxation, degeneration, bony proliferation, capsular/ligamentous hypertrophy or fracture can irritate the common dorsal ramus and medial branch, and induce clinical symptoms [18,44,47,48]. Ossification of the mammilloaccessory ligament may cause an entrapment neuropathy and low back pain [18,24,33].
Chen and colleagues [51] dissected the spinal dorsal rami from T12 to the sacrum and conducted biomechanical studies. Their study demonstrated that the L2 dorsal rami bore the greatest stretching force and tensile stress when the specimens were flexed and rotated to the contralateral side.
Spinal dorsal ramus mediated back pain can occur at any level of the human spine [18,21,22,44,52,53]. For low back pain mediated by dorsal ramus, the primary pain is commonly at the thoracolumbar junction [19-22, 38,44]. Within the thoracic region, the coronal orientation of the zygapophysial joints grants spine free rotation. However, this rotation is limited by a rigid rib cage, except at the T10-12 levels because of floating ribs. The upper lumbar facets also have a relative coronal orientation. Therefore, spine rotation is relatively free at the thoracolumbar junction and the greatest shear force occurs at the more mobile upper lumbar segments. This normal spinal movement can cause zygapophysial joint separation or rotation. If these movements occur rapidly or overcome the body’s physiological limit, they can cause stretching tension and irritation to the dorsal ramus, resulting in low back pain [20,40,44,54]. Shao and his colleagues reported that seventy four percent (74%) of the 1263 patients with spinal dorsal ramus mediated low back pain had the pain originating from L1 and/or L2 dorsal ramus [36].
http://file.scirp.org/Html/9-2400120/3fe33e99-0bf8-4fbf-ac3c-867b9de28c6b.jpg
Additionally, Zhou has reported in his retrospective study, that in 41 patients with spinal dorsal ramus mediated lower back pain, after the selective spinal dorsal ramus injection, 84% of these patients received greater than 50% and more than two months of pain reduction [74]. These patients also reported improvement in their daily activities and decrease of their pain medications [74].
Normally, this type of pain originates at L1 or L2 dorsal rami, and the pathogeneses can be multiple factors which irritate the dorsal ramus. The back pain induced by dorsal ramus irritation can occur in the cervical [51] and thoracic spine [50] as well. Therefore, spinal dorsal ramus mediated back pain should be appropriately called “spinal dorsal ramus syndrome (SDRS)”.
The clinical presentations of dorsal ramus mediated back pain and zygapophysial syndrome can be overlapping. However, there are some distinctions. The thoracolumbar junction is the most common site of spinal dorsal ramus mediated back pain [21,22,36], while, zygapophysial joint syndrome commonly occurs at the lower lumbar zygapophysial joints such as L5-S1 and L4-5 [5,6,9,43,57, 58].
Spennede studie som nevner mange viktige prinsipper rundt CO2 og hinter til at det er veldig mye vi har misforstått.
Beskriver spesielt godt hvordan lav CO2 (alkalose) gjør at cellemembraner blir mer permeabal (slipper ting lettere igjennom) for å balansere pH inne i cellen. Noe som fører til at også Ca2+ slippes inn i cellene og f.eks. muskelceller trekker seg mer sammen og nerveceller fyrer av lettere. Kroppen trenger mer oksygen og den setter igang en negativ spiral hvor økt pustefrekvens gir mindre CO2 som gir mer behov for oksygen og dermed en videreføing av økt pustefrekvens. Høy CO2 (acidose) gjør det motsatte, muskler slapper av, nervene roes ned og cellen beskyttes.
http://www.ncbi.nlm.nih.gov/pubmed/20128395
Hele studien: http://www.mppt.hu/images/magazin/pdf/xi-evfevfolyam-3-szam/a-szendioxid-es-az-intracellularis-ph.pdf
The role of carbon dioxide (CO2) is underestimated in the pathomechanism of neuropsychiatric disorders, though it is an important link between psyche and corpus.
The actual spiritual status also influences respiration (we start breathing rarely, frequently, irregularly, etc.) causing pH alteration in the organism;
on the other hand the actual cytosolic pH of neurons is one of the main modifiers of Ca2+-conductance, hence breathing directly, quickly, and effectively influences the second messenger system through Ca2+-currents. (Decreasing pCO2 turns pH into alkalic direction, augments psychic arousal, while increasing pCO2 turns pH acidic, diminishes arousal.)
One of the most important homeostatic function is to maintain or restore the permanence of H+-concentration, hence the alteration of CO2 level starts cascades of contraregulation. However it can be proved that there is no perfect compensation, therefore compensational mechanisms may generate psychosomatic disorders causing secondary alterations in the «milieu interieur».
Authors discuss the special physico-chemical features of CO2, the laws of interweaving alterations of pCO2 and catecholamine levels (their feedback mechanism), the role of acute and chronic hypocapnia in several hyperarousal disorders (delirium, panic disorder, hyperventilation syndrome, generalized anxiety disorder, bipolar disorder), the role of «locus minoris resistentiae» in the pathomechanism of psychosomatic disorders. It is supposed that the diseases of civilization are caused not by the stress itself but the lack of human instinctive reaction to it, and this would cause long-lasting CO2 alteration. Increased brain-pCO2, acidic cytosol pH and/or increased basal cytosolic Ca2+ level diminish inward Ca2+-current into cytosol, decrease arousal–they may cause dysthymia or depression. This state usually co-exists with ATP-deficiency and decreased cytosolic Mg2+ content. This energetical- and ion-constellation is also typical of ageing-associated and chronic organic disorders. It is the most important link between depression and organic disorders (e.g. coronary heart disease). The above-mentioned model is supported by the fact that H+ and/or Ca2+ metabolism is affected by several drugs (catecholemines, serotonin, lithium, triaecetyluridine, thyroxine) and sleep deprivation, they act for the logically right direction.
If we take our breath deeply or frequently our pulse speeds up proving that CO2 has left the pacemaker cells of heart, and the alkalic cytoplasm allowes Ca2+ to enter in the cytosol. If we keep on this kind of breathing for a long time, our pulse will slowly come back to the incipient frequency because the organism compensates the alteration of pH in the cytosol. The lack of H+ in cytosol increases conductance of Ca 2+ and some other ions (Harvey et al.), thus it increases contraction, metabolism and O2 requirement (Laffey et al.), and also increases excitability of neurons in the peripherium (Macefield et al.) and in the brain (Stenkamp et al.). All these events can be explained by the simple fact that lack of H+ (=alkalosis) increases transmembrane conductance of ions and (consequently) increases active ion-pumping mechanisms too (because the original ion-status has to be restored). By contrast, acidosis decreases the transmembrane Ca 2+-conductance (Tombaugh & Somjen), decreases excitability of neurons, and the decreased Ca 2+-conductance can dramatically affect neurotransmitter re- lease (Dodge et al..).
Then chronic hypocapnia or hypercapnia is followed by cascades which alter the whole ionmileu in the cells, they may alter even the neurotransmitter/endocrine sta- tus (Dodge et al.). Therefore, it is inappropriate to call that process a “compensational mechanism”, this name suggests that it is all right, while it is not! According to Claude Bernard alteration of milieu interieur can result in illness. It is very important that the new ion milieu is similarly stable as the original one and it does not allow the organism to restore the original status. Therefore we should name this happening a „complication” (in- stead of “compensation”).
ALLE (!!!) muskel- og ledd terapeuter tar først og fremst på huden. Og ALLE gjør alt de kan for å overse det. Vi kan trygt si at huden er undervurdert i behandling av menneskekroppen. Spesielt siden ALLE behandlingseffekter egentlig er sekundæreffekter av det som skjer i hudens nervesystem og hjernens opplevelse av dette.
Huden er vårt største organ. Og vårt mest sensitive organ. Det er så tettpakket av sensoriske nervetråder at vi kan si den er «utsiden av hjernen». Vi er faktisk så godt beskyttet av huden at det er kun hjernens opplevelse av det som skjer med huden som avgjør hva som skjer med vevet under huden. Alle som tar på huden i en behandlingssituasjon er fullstendig underlagt nervesystemets reaksjon på berøringen.
Muskler, ledd og bindevev gjør bare det nervesystemet befaler. Når vi vet hvilken direkte kobling huden har til nervesystemet og hjernen kan vi også rette behandlingskonseptene våre direkte på det som faktisk gir behandlingseffekt: Nervesystemet
Når vi trykker på et triggerpunkt, et ømt område av en muskel, så finnes det svært få trykksensitive nerver i selve muskelen. De finnes hovedsaklig i huden og vevet rett under huden. Smerten vi opplever av trykket kommer altså ikke av at vi trykker på muskelen, men at vi trykker på huden. Selv om det kjennes ut som at vi trykker hardt og dypt inn vevet, så er det hudens nerver som reagerer på trykket. Om vi bedøver hudens nerver når vi f.eks. er støle, så forsvinner trykksensitiviteten også. Når vi jobber med å dempe smerte trenger vi altså ikke trykke hardt inn i muskelen, vi trenger bare å ha en litt smartere tilnærming til huden.
Smerte er en subjektiv opplevelse som er ment å beskytte kroppen. Det innebærer et tett samarbeid mellom hjernens registrering av faresignaler fra huden og dens interne kart over kroppen. Fra et evolusjonært perspektiv er det større farer i omgivelsene enn internt i kroppen. Derfor dekker de fare-registrerende nervene (nociceptorer) hele kroppens overflate. Det er også noe av grunnen til at vi føler oss trygge og slapper bedre av når noen tar på huden vår på en behagelig og ikke-truende måte.
Det krever en ganske stor omveltning for å innse hudens rolle i smertebehandling. Det er veldig mye som vi tidligere har tatt for gitt som må snus på hodet. Vi må lære oss å legge merke til noe medisinsk vitenskap har brukt 200 år på å overse.
Med en helt ny forståelse av menneskekroppen og behandling av nervesystemet kan vi også behandle smertetilstander direkte, men uten å gi ny smerte slik de «gamle» behandlingsformene gjør. De som overser huden, vårt største og viktigste sanseorgan, og (håpløst) prøver å trykke fingrene igjennom den.
Med den nye behandlingsformen DermoNeuroModulation snur vi alt på hodet og behandler smerte UTEN å gi ny smerte. Når vi vet hvordan huden og nervesystemet fungerer trenger vi kun å gi en behagelig og interaktiv behandling av huden, og smerte dempes umiddelbart.

{kind=link}
{kind=link}
{kind=link}
{kind=link}