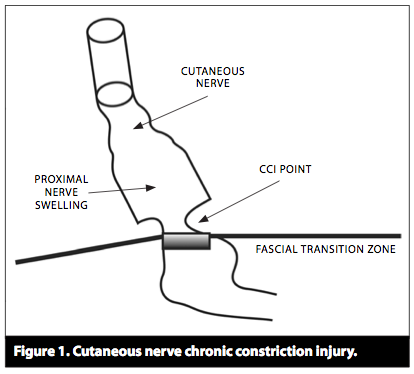
En studie til fra Siegfried Mense, om muskelsmerter. Han har ikke fått med seg at trykksensitive nerver kun finnes i huden. Og han har misforstått litt i forskjellene mellom hud-smerter og muskel-smerter siden han sier at hud-smerter ikke kan ha utstrålende effekt. Han har tydeligvis ikke ikke inkludert subcutane nerver i sin vurdering.
Men mye interessant i denne studien likevel. Spesielt vektleggingen av at lav pH er den viktigste bidragsyteren til muskelsmerter.
Han nevner at input fra muskel-nociceptorer har større relevans i ryggmargen enn input fra huden. Derfor er betennelser og lav pH de viktigste drivkreftene i kroniske smerter.
Nevner også at smerter henger sammen, f.eks. at trapezius kan stramme seg for å beskytte brachialis, slik at smerten kjennes i trapezius, mens problemet egentlig sitter i brachialis.
Beskriver også triggerpunkter, men sier at det foreløpig er veldig mange ubesvarte spørsmål om denne teorien.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2696782
Muscle pain is a major medical problem: in, the majority (60% to 85%) of the population has had (nonspecific) back pain of muscular origin at some time or other (lifetime prevalence) (1). Pain evoked by myofascial trigger points has a point prevalence of approximately 30% (2). More than 7% of all women aged 70 to 80 years suffer from the fibromyalgia syndrome (e1). In an Italian study, musculoskeletal pain was found to be the most common reason that patients consulted a doctor (3). Thus, treating physicians should be aware of the mechanisms of muscle pain, insofar as they are currently understood.
Subjective differences between muscle pain and cutaneous pain
| Muscle pain | Cutaneous pain |
| Electrical nerve stimulation induces only one pain | Electrical nerve stimulation induces a first pain and a second pain |
| Poorly localizable | Well-localized |
| Tearing, cramping, pressing quality | Stabbing, burning, cutting quality |
| Marked tendency toward referral of pain | No tendency toward referral of pain |
| Affective aspect: difficult to tolerate | Affective aspect: easier to tolerate |
Muscle pain is produced by the activation of specific receptors (so-called nociceptors): these receptors are specialized for the detection of stimuli that are objectively capable of damaging tissue and that are subjectively perceived as painful. They consist of free nerve endings and are connected to the central nervous system (CNS) by way of unmyelinated (group IV) or thinly myelinated (group III) fibers. They can be sensitized and activated by strong mechanical stimuli, such as trauma or mechanical overloading, as well as by endogenous inflammatory mediators including bradykinin (BK), serotonin, and prostaglandin E2 (PGE2).
Two activating chemical substances are particularly important for the generation of muscle pain: adenosine triphosphate (ATP) and protons (H+ ions).
ATP activates muscle nociceptors mainly by binding to the P2X3 receptor molecule, H+ mainly by binding to the receptor molecules TRPV1 (transient receptor potential vanilloid 1) and ASICs (acid-sensing ion channels) (4).
ATP is found in all cells of the body and is released whenever bodily tissues of any type are injured.
A drop in pH is probably one of the main activators of peripheral nociceptors, as many painful disturbances of muscle are associated with low pH in muscle tissue.
Nerve growth factor (NGF) also has a connection to muscle pain: NGF is synthesized in muscle and activates muscle nociceptors (e2). NGF synthesis is increased when a muscle is inflamed (e3).
Acidic tissue pH is one of the main activating factors leading to muscle pain. Practically all pathological and pathophysiological changes of skeletal muscle are accompanied by a drop in pH, among them
- chronic ischemic states,
- tonic contractions or spasms,
- myofascial trigger points,
- (occupationally induced) postural abnormalities, and
- myositides.
The neuropeptides stored in muscle nociceptors are released not only when peripheral stimuli activate the nerve endings, but also when spinal nerves are compressed. In this type of neuropathic pain, action potentials are generated at the site of compression and spread not only centripetally, i.e., toward the central nervous system, but also centrifugally, i.e., toward the nociceptive endings, where they induce the release of vasoactive neuropeptides. In this way, neurogenic inflammation comes about, characterized by hyperemia, edema, and the release of inflammatory mediators (8). The inflammatory mediators sensitize the muscle nociceptors and thereby increase neuropathic pain.
The sensitization of the muscle nociceptors by endogenous mediators such as BK and PGE2 is one of the reasons why patients with muscle lesions suffer from tenderness to pressure on the muscle, and from pain on movement or exercise. It is also the reason why many types of muscle pain respond well to the administration of non-steroidal anti-inflammatory drugs (NSAID), which block prostaglandin synthesis.
An influx of nervous impulses from muscle nociceptors into the spinal cord increases the excitability of posterior horn neurons to a greater extent than one from cutaneous nociceptors (9).
Two main mechanisms underlie the overexcitability of spinal nociceptive neurons:
A structural change of ion channels, rendering them more permeable to Na+ and Ca2+, is the short-term result of an influx of nociceptive impulses into the spinal cord. Among other effects, this causes originally ineffective («silent» or «dormant») synapses to become effective.
A change of gene transcription in the neuronal nucleus, leading to a modification of synthetic processes, causes new ion channels to be synthesized and incorporated into the nerve cell membrane. The long-term result of central sensitization is a nociceptive cell whose membrane contains a higher density of ion channels that are also more permeable to ions. This explains the hyperexcitability of the cell. Glial cells, too, particularly microglia, can contribute to the sensitization of central neurons by secreting substances such as tumor necrosis factor a (TNF-a) (8).
The increased excitability of spinal neurons and the spread of excitation within the CNS are the first steps in the process of chronification of muscle pain. The endpoint of chronification consists of structural remodeling processes in the CNS that open up new pathways for nociceptive information and cause pain to persist over the long term. Patients with chronic muscle pain are difficult to treat, because the functional and structural changes in the CNS need time to regress. The fact that not all muscle pain becomes chronic implies that chronification requires not only the mechanisms just discussed, but also other ones, e.g., a genetic predisposition.
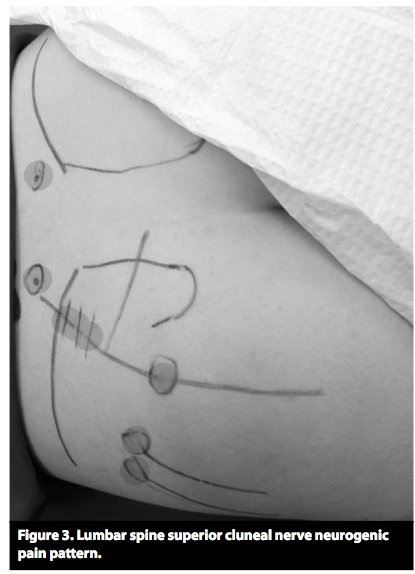
Pain arising in muscle is more likely to be referred pain than pain arising in the skin. Referred pain is pain that is felt not (only) at its site of origin, but at another site some distance away. A possible mechanism of referred pain is the spread, within the spinal cord, of excitation due to the muscle lesion (9) (figures 2 and and3).3). As soon as the excitation reaches sensory posterior horn neurons that innervate an area beyond the site of the original muscle lesion, the patient feels referred pain in that area, even though none of the nociceptors in it are activated (13).

An example is shown in figure 3: a stimulus delivered to the myofascial trigger point (MTrP) in the soleus muscle causes only mild local pain, while the patient feels more severe (referred) pain in the sacroiliac joint. No conclusive answers are yet available to the questions of why muscle pain is more likely than cutaneous pain to be referred, why it is usually not referred to both proximal and distal sites, and why pain referral is often discontinuous. There is, however, a well-known discontinuity of spinal topography between the C4 and T2 dermatomes.
The main reason why pain arises in muscle spasm is muscle ischemia, which leads to a drop in pH and the release of pain-producing substances such as bradykinin, ATP, and H+.
The vicious-circle concept of muscle spasm – muscle pain causes spasm, which causes more pain, etc. – should now be considered obsolete. Most studies have shown that muscle pain lowers the excitability of the α-motor neurons innervating the painful muscle (14) (a «pain adaptation» model) (15).
Muscle spasm can be precipitated by, among other things, pain in another muscle. Thus, a spasm-like increase EMG activity in the trapezius muscle has been described in response to painful stimulation of the biceps brachii muscle (16). Another source of muscle spasms is pathological changes in a neighboring joint. These sources of pain must be deliberately sought.
In a widespread hypothesis on the origin of MTrP’s (19), it is supposed that a muscular lesion damages the neuromuscular endplate so that it secretes an excessive amount of acetylcholine. The ensuing depolarization of the muscle cell membrane produces a contraction knot that compresses the neighboring capillaries, causing local ischemia. Ischemia, in turn, leads to the release of substances into the tissue that sensitize nociceptors, accounting for the tenderness of MTrP’s to pressure. Substances of this type have been found to be present within the MTrP’s of these patients (20). This supposed mechanism leaves many questions unanswered but is currently the only comprehensive hypothesis on the origin of MTrP’s.
Patients with MTrP’s often have pain in three locations:
- at the site of the MTrP itself,
- at the origin or insertion of the affected muscle, because of pulling by the muscle fibers that have been stretched by the contraction knots,
- and referred pain outside the MTrP (figure 3).
Because the MTrP is cut off from its blood supply by compression of the local microcirculation, oral NSAID’s are not very effective against TrP pain.
 Muskelspenninger helt øverst i nakken bidrar til mange problemer. F.eks. hodepine, spenningsmigrene, kjevespenning, nakkeplager, bevegelsessmerter i nakken, dårlig søvn, m.m.. Spesielt smerter i panna og tinningene har ofte utgangspunkt i området øverst i nakken.
Muskelspenninger helt øverst i nakken bidrar til mange problemer. F.eks. hodepine, spenningsmigrene, kjevespenning, nakkeplager, bevegelsessmerter i nakken, dårlig søvn, m.m.. Spesielt smerter i panna og tinningene har ofte utgangspunkt i området øverst i nakken.