Stikkordarkiv: Nervesystemet
Structure of the rat subcutaneous connective tissue in relation to its sliding mechanism.
Om hvordan bindevevet i huden beveger seg når man strekker huden. Nevner at nerver og blodårer har veldig svingete baner i huden, og at dette gjør at vi tåler mye strekk og bevegelse uten at disse strekkes eller ødelegges.
http://www.ncbi.nlm.nih.gov/pubmed/14527168/
The subcutaneous connective tissue was observed to be composed of multiple layers of thin collagen sheets containing elastic fibers. These piled-up collagen sheets were loosely interconnected with each other, while the outer and inner sheets were respectively anchored to the dermis and epimysium by elastic fibers. Collagen fibers in each sheet were variable in diameter and oriented in different directions to form a thin, loose meshwork under conditions without mechanical stretching.
When a weak shear force was loaded between the skin and the underlying abdominal muscles, each collagen sheet slid considerably, resulting in a stretching of the elastic fibers which anchor these sheets. When a further shear force was loaded, collagen fibers in each sheet seemed to align in a more parallel manner to the direction of the tension. With the reduction or removal of the force, the arrangement of collagen fibers in each sheet was reversed and the collagen sheets returned to their original shapes and positions, probably with the stabilizing effect of elastic fibers.
Blood vessels and nerves in the subcutaneous connective tissue ran in tortuous routes in planes parallel to the unloaded skin, which seemed very adaptable for the movement of collagen sheets. These findings indicate that the subcutaneous connective tissue is extensively mobile due to the presence of multilayered collagen sheets which are maintained by elastic fibers.
Immunohistochemical analysis of wrist ligament innervation in relation to their structural composition.
Nevner at noen ligamenter i håndleddethar mye innervasjon og er viktige for propriosepsjon, mens andre har ikke det. Sier at innervasjonen sitter helt ytterst i ligamentene. Nevner at det meste av innerverte ligamenter er på oversiden.
http://www.ncbi.nlm.nih.gov/pubmed/17218173/
The innervation pattern in the ligaments was found to vary distinctly, with a pronounced innervation in the dorsal wrist ligaments (dorsal radiocarpal, dorsal intercarpal, scaphotriquetral, dorsal scapholunate interosseous), an intermediate innervation in the volar triquetral ligaments (palmar lunotriquetral interosseous, triquetrocapitate, triquetrohamate), and only limited/occasional innervation in the remaining volar wrist ligaments. The innervation pattern also was reflected in the structural differences between the ligaments.
When present, mechanoreceptors and nerve fibers were consistently found in the loose connective tissue in the outer region (epifascicular region) of the ligament. Hence, ligaments with abundant innervation had a large epifascicular region, as compared with the ligaments with limited innervation, which consisted mostly of densely packed collagen fibers.
The results of our study suggest that wrist ligaments vary with regard to sensory and biomechanical functions. Rather, based on the differences found in structural composition and innervation, wrist ligaments are regarded as either mechanically important ligaments or sensory important ligaments. The mechanically important ligaments are ligaments with densely packed collagen bundles and limited innervation. They are located primarily in the radial, force-bearing column of the wrist. The sensory important ligaments, by contrast, are richly innervated although less dense in connective tissue composition and are related to the triquetrum. The triquetrum and its ligamentous attachments are regarded as key elements in the generation of the proprioceptive information necessary for adequate neuromuscular wrist stabilization.

The fascia of the limbs and back – a review
Never det meste rundt bindevev: tensegritet, subcutan hud, skinligaments, stretching, ligamenter, nerver, m.m.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2667913/
Fasciae probably hold many of the keys for understanding muscle action and musculoskeletal pain, and maybe of pivotal importance in understanding the basis of acupuncture and a wide range of alternative therapies (Langevin et al. 2001, 2002, 2006a; Langevin & Yandow, 2002; Iatridis et al. 2003). Intriguingly, Langevin et al. (2007) have shown that subtle differences in the way that acupuncture needles are manipulated can change how the cells in fascia respond. The continuum of connective tissue throughout the body, the mechanical role of fascia and the ability of fibroblasts to communicate with each other via gap junctions, mean that fascia is likely to serve as a body-wide mechanosensitive signaling system with an integrating function analogous to that of the nervous system (Langevin et al. 2004; Langevin, 2006). It is indeed a key component of a tensegrity system that operates at various levels throughout the body and which has been considered in detail by Lindsay (2008) in the context of fascia.
Anatomists have long distinguished between superficial and deep fascia (Fig. 1), although to many surgeons, ‘fascia’ is simply ‘deep fascia’. The superficial fascia is traditionally regarded as a layer of areolar connective or adipose tissue immediately beneath the skin, whereas deep fascia is a tougher, dense connective tissue continuous with it.

A diagrammatic representation of a transverse section through the upper part of the leg showing the relative positions of the superficial (SF) and deep fascia (DF) in relation to the skin (S) and muscles. Note how the deep fascia, in association with the bones [tibia (T) and fibula (F)] and intermuscular septa (IS) forms a series of osteofascial compartments housing the extensor, peroneal (PER) and flexor muscles. If pressure builds up within a compartment because of an acute or overuse injury, then the vascular supply to the muscles within it can be compromised and ischaemia results. ANT, anterior compartment; IM, interosseous membrane.
The presence of a significant layer of fat in the superficial fascia is a distinctive human trait (thepanniculus adiposus), compensating for the paucity of body hair. It thus plays an important role in heat insulation. In hairy mammals, the same fascia is typically an areolar tissue that allows the skin to be readily stripped from the underlying tissues (Le Gros Clark, 1945). Where fat is prominent in the superficial fascia (as in man), it may be organized into distinctive layers, or laminae (Johnston & Whillis, 1950), although Gardner et al. (1960) caution that these may sometimes be a characteristic of embalmed cadavers and not evident in the living person. Furthermore, Le Gros Clark (1945) also argues that fascial planes can be artefactually created by dissection. Conversely, however, some layers of deep fascia are more easily defined in fresh than in fixed cadavers (Lytle, 1979).
The superficial fascia conveys blood vessels and nerves to and from the skin and often promotes movement between the integument and underlying structures.
Skin mobility protects both the integument and the structures deep to it from physical damage. Mobility is promoted by multiple sheets of collagen fibres coupled with the presence of elastin (Kawamata et al. 2003). The relative independence of the collagen sheets from each other promotes skin sliding and further stretching is afforded by a re-alignment of collagen fibres within the lamellae. The skin is brought back to its original shape and position by elastic recoil when the deforming forces are removed. As Kawamata et al. (2003)point out, one of the consequences of the movement-promoting characteristics of the superficial fascia is that the blood vessels and nerves within it must run a tortuous route so that they can adapt to an altered position of the skin, relative to the deeper structures.
Although deep fascia elsewhere in the limbs is often not so tightly bound to the skin, nevertheless cutaneous ligaments extending from deep fascia to anchor the integument are much more widespread than generally recognized and serve to resist a wide variety of forces, including gravitational influences (Nash et al. 2004).
According to Bouffard et al. (2008), brief stretching decreases TGF-β1-mediated fibrillogenesis, which may be pertinent to the deployment of manual therapy techniques for reducing the risk of scarring/fibrosis after an injury. As Langevin et al. (2005) point out, such striking cell responses to mechanical load suggest changes in cell signaling, gene expression and cell-matrix adhesion.
In contrast, Schleip et al. (2007) have reported myofibroblasts in the rat lumbar fascia (a dense connective tissue). The cells can contract in vitro andSchleip et al. (2007) speculate that similar contractions in vivo may be strong enough to influence lower back mechanics. Although this is an intriguing suggestion that is worthy of further exploration, it should be noted that tendon cells immunolabel just as strongly for actin stress fibres as do fascial cells and this may be associated with tendon recovery from passive stretch (Ralphs et al. 2002). Finally, the reader should also note that true muscle fibres (both smooth and skeletal) can sometimes be found in fascia. Smooth muscle fibres form the dartos muscle in the superficial fascia of the scrotum and skeletal muscle fibres form the muscles of fascial expression in the superficial fascia of the head and neck.
Consequently, entheses are designed to reduce this stress concentration, and the anatomical adaptations for so doing are evident at the gross, histological and molecular levels. Thus many tendons and ligaments flare out at their attachment site to gain a wide grip on the bone and commonly have fascial expansions linking them with neighbouring structures. Perhaps the best known of these is the bicipital aponeurosis that extends from the tendon of the short head of biceps brachii to encircle the forearm flexor muscles and blend with the antebrachial deep fascia (Fig. 6). Eames et al. (2007) have suggested that this aponeurosis may stabilize the tendon of biceps brachii distally. In doing so, it reduces movement near the enthesis and thus stress concentration at that site.

The bicipital aponeurosis (BA) is a classic example of a fascial expansion which arises from a tendon (T) and dissipates some of the load away from its enthesis (E). It originates from that part of the tendon associated with the short head of biceps brachii (SHB) and blends with the deep fascia (DF) covering the muscles of the forearm. The presence of such an expansion at one end of the muscle only, means that the force transmitted through the proximal and distal tendons cannot be equal. LHB, long head of biceps brachii. Photograph courtesy of S. Milz and E. Kaiser.
Several reports suggest that fascia is richly innervated, and abundant free and encapsulated nerve endings (including Ruffini and Pacinian corpuscles) have been described at a number of sites, including the thoracolumbar fascia, the bicipital aponeurosis and various retinacula (Stilwell, 1957; Tanaka & Ito, 1977; Palmieri et al. 1986; Yahia et al. 1992; Sanchis-Alfonso & Rosello-Sastre, 2000; Stecco et al. 2007a).
Changes in innervation can occur pathologically in fascia, and Sanchis-Alfonso & Rosello-Sastre (2000) report the ingrowth of nociceptive fibres, immunoreactive to substance P, into the lateral knee retinaculum of patients with patello-femoral malignment problems.
Stecco et al. (2008) argue that the innervation of deep fascia should be considered in relation to its association with muscle. They point out, as others have as well (see below in ‘Functions of fascia’) that many muscles transfer their pull to fascial expansions as well as to tendons. By such means, parts of a particular fascia may be tensioned selectively so that a specific pattern of proprioceptors is activated.
It is worth noting therefore that Hagert et al. (2007) distinguish between ligaments at the wrist that are mechanically important yet poorly innervated, and ligaments with a key role in sensory perception that are richly innervated. There is a corresponding histological difference, with the sensory ligaments having more conspicuous loose connective tissue in their outer regions (in which the nerves are located). Comparable studies are not available for deep fascia, although Stecco et al. (2007a) report that the bicipital aponeurosis and the tendinous expansion of pectoralis major are both less heavily innervated than the fascia with which they fuse. Where nerves are abundant in ligaments, blood vessels are also prominent (Hagert et al. 2005). One would anticipate similar findings in deep fascia.
Some of the nerve fibres associated with fascia are adrenergic and likely to be involved in controlling local blood flow, but others may have a proprioceptive role. Curiously, however, Bednar et al. (1995)failed to find any nerve fibres in thoracolumbar fascia taken at surgery from patients with low back pain.
The unyielding character of the deep fascia enables it to serve as a means of containing and separating groups of muscles into relatively well-defined spaces called ‘compartments’.
One of the most influential anatomists of the 20th century, Professor Frederic Wood Jones, coined the term ‘ectoskeleton’ to capture the idea that fascia could serve as a significant site of muscle attachment – a ‘soft tissue skeleton’ complementing that created by the bones themselves (Wood Jones, 1944). It is clearly related to the modern-day concept of ‘myofascia’ that is popular with manual therapists and to the idea of myofascial force transmission within skeletal muscle, i.e. the view that force generated by skeletal muscle fibres is transmitted not only directly to the tendon, but also to connective tissue elements inside and outside the skeletal muscle itself (Huijing et al. 1998; Huijing, 1999).
One can even extend this idea to embrace the concept that agonists and antagonists are mechanically coupled via fascia (Huijing, 2007). Thus Huijing (2007) argues that forces generated within a prime mover may be exerted at the tendon of an antagonistic muscle and indeed that myofascial force transmission can occur between all muscles of a particular limb segment.
Wood Jones (1944) was particularly intrigued by the ectoskeletal function of fascia in the lower limb. He related this to man’s upright stance and thus to the importance of certain muscles gaining a generalized attachment to the lower limb when it is viewed as a whole weight-supporting column, rather than a series of levers promoting movement. He singled out gluteus maximus and tensor fascia latae as examples of muscles that attach predominantly to deep fascia rather than bone (Wood Jones, 1944).
They have argued that a common attachment to the thoracolumbar fascia means that the latter has an important role in integrating load transfer between different regions. In particular, Vleeming et al. (1995) have proposed that gluteus maximus and latissimus dorsi (two of the largest muscles of the body) contribute to co-ordinating the contralateral pendulum like motions of the upper and lower limbs that characterize running or swimming. They suggest that the muscles do so because of a shared attachment to the posterior layer of the thoracolumbar fascia. Others, too, have been attracted by the concept of muscle-integrating properties of fascia. Thus Barker et al. (2007) have argued for a mechanical link between transversus abdominis and movement in the segmental neutral zone of the back, via the thoracolumbar fascia. They feel that the existence of such fascial links gives an anatomical/biomechanical foundation to the practice in manual therapy of recommending exercises that provoke a submaximal contraction of transversus abdominis in the treatment of certain forms of low back pain.
An important function of deep fascia in the limbs is to act as a restraining envelope for muscles lying deep to them. When these muscles contract against a tough, thick and resistant fascia, the thin-walled veins and lymphatics within the muscles are squeezed and their unidirectional valves ensure that blood and lymph are directed towards the heart. Wood Jones (1944) contests that the importance of muscle pumping for venous and lymphatic return is one of the reasons why the deep fascia in the lower limb is generally more prominent than in the upper – because of the distance of the leg and foot below the heart.
In certain regions of the body, fascia has a protective function. Thus, the bicipital aponeurosis (lacertus fibrosus), a fascial expansion arising from the tendon of the short head of biceps brachii (Athwal et al. 2007), protects the underlying vessels. It also has mechanical influences on force transmission and stabilizes the tendon itself distally (Eames et al. 2007).
Immunohistochemical demonstration of nerve endings in iliolumbar ligament.
Ett par studier som bekrefter at IL ligamentet er fullt av nervetråder. Viktig å vite for ligamentbehandlingen vi gjør på Verkstedet.
http://www.ncbi.nlm.nih.gov/pubmed/20081564
The function of iliolumbar ligament and its role in low back pain has not been yet fully clarified. Understanding the innervation of this ligament should provide a ground which enables formation of stronger hypotheses.
Iliac wing insertion was found to be the richest region of the ligament in terms of mechanoreceptors and nociceptors. Pacinian (type II) mechanoreceptor was determined to be the most common (66.67%) receptor followed by Ruffini (type I) (19.67%) mechanoreceptor, whereas free nerve endings (type IV) and Golgi tendon organs (type III) were found to be less common, 10.83% and 2.83%, respectively.
Those results indicate that ILL plays an important role in proprioceptive coordination of lumbosacral region alongside its known biomechanic support function. Moreover, the presence of type IV nerve endings suggest that the injury of this ligament might contribute to the low back pain.
Mer om IL ligamentet i denne studien:
Sensory innervation of the thoracolumbar fascia in rats and humans.
Studie som viser innervasjon av korsryggbindevev og påpeker at det er kun det ytre laget av bindevevet, det som er helt inn mot huden, som er tettpakket med sensoriske nerver og nociceptive fibre (som utskiller substans P og CGRP, og gir betennelser). De dypere lagene i midten av bindevevet eller ned mot musklene har nesten ingen nerveender eller sansesmuligheter.
http://www.ncbi.nlm.nih.gov/pubmed/21839150
Hele studien i min dropbox.
The subcutaneous tissue and the outer layer showed a particularly dense innervation with sensory fibers. SP-positive free nerve endings-which are assumed to be nociceptive-were exclusively found in these layers. Because of its dense sensory innervation, including presumably nociceptive fibers, the TLF may play an important role in low back pain.

Fig. 1. Structure of the rat thoracolumbar fascia (TLF) close to the spinous processes L4/L5. (a) Transversal section showing the three layers of the TLF (hematoxylin and eosin staining): OL, outer layer with transversely oriented collagen fibers; ML, middle layer composed of collagen fiber bundles oriented diagonally to the long axis of the body; IL, inner layer of loose connective tissue covering the multifidus muscle (muscle). SCT, subcutaneous tissue. (b) PGP 9.5-ir nerve fibers in the layers of the TLF. Black arrows, fibers on passage; open arrows, nerve endings. (c) Mean fiber length of PGP 9.5-ir fibers in the TLF. The great majority of all fibers were located in the outer layer (OL) of the fascia and in the subcutaneous tissue (SCT). White part of the bar: subcutaneous tissue plus outer layer of the TLF; black: middle layer; hatched: inner layer. n, number of sections evaluated.

Fig. 4. Distribution of CGRP and Substance P (SP)-immunoreactive nerve fibers in the TLF. (a) Mean fiber length of CGRP-ir nerve fibers. (b) Mean fiber length of SP-ir nerve fibers. Almost all fibers were found in the outer layer of the fascia and the subcutaneous tissue. The middle layer was free of SP-positive fibers. Gray part of the bars: subcutaneous tissue; white: outer layer of the TLF; black: middle layer; hatched: inner layer. n=number of sections evaluated. (c, d) Distribution of CGRP- (c) and SP-containing receptive free nerve endings (d) expressed as percent of the total number of CGRP- or SP-containing fibers in each layer. For classification as receptive endings, the structures had to exhibit at least three varicosities. SP-containing free nerve endings were restricted to the outer layer of the thoracolumbar fascia and the subcutaneous connective tissue while CGRP-containing free nerve endings were also found in the inner layer of the thoracolumbar fascia.
Og et bilde av de forskjellige bindevevslagene som er nevnt i denne studien.

Our study demonstrates that the rat TLF and the SCT overlying the fascia are densely innervated tissues, and therefore both the TLF and SCT, may play a role in low back pain. Most nerve fibers are located in the OL of the TLF and in the SCT, whereas in the ML nerve fibers are rare. Actually, no SP-ir fibers were found in this layer. Teleologically, the lack of fibers in the ML, particularly those containing SP, makes sense because each move- ment of the body causes shearing forces between the collagen fiber bundles, which might excite nociceptors.
Entrapment Neuropathies in the Upper and Lower Limbs: Anatomy and MRI Features
Nevner viktige steder nerver kommer i klem.
http://www.hindawi.com/journals/rrp/2012/230679/
Although nerves may be injured anywhere along their course, peripheral nerve compression or entrapment occurs more at specific locations, such as sites where a nerve courses through fibroosseous or fibromuscular tunnels or penetrates muscles [2, 3].

Figure 1: The drawing shows anatomy of the suprascapular nerve from the posterior view. Note the nerve courses through the suprascapular notch (open arrow) and spinoglenoid notch (curved arrow). SSN: suprascapular nerve, SS: supraspinatus muscle, IS: infraspinatus muscle.
Suprascapular nerve compression or entrapment, known as suprascapular nerve syndrome, can occur as a result of trauma, an anomalous or thickened transverse scapular ligament, or extrinsic compression by a space-occupying lesion [7, 8], commonly a ganglia cyst or soft tissue tumor. Compression or entrapment at the suprascapular notch leads to supraspinatus and infraspinatus muscle denervation (Figure 2), whereas more distal entrapment at the spinoglenoid notch may present with isolated involvement of the infraspinatus muscle (Figure 3). Patients may present with poorly localized pain and discomfort at the back of the shoulder or the upper back, as well as weakness when raising the arm.

Figure 4: The drawing shows the axillary nerve within the quadrilateral space from a posterior view. AN: axillary nerve, Tm: teres minor muscle, Tr: long head of the triceps, TM: teres major muscle, H: humerus, D: deltoid muscle.
Clinical manifestations include poorly localized shoulder pain and paresthesias in the affected arm in a nondermatomal distribution. The diagnosis can be difficult since clinical symptoms may be confused with rotator cuff pathology or other shoulder joint-related abnormalities [9].

Figure 6: The drawing provides an anterior view of the course of the radial nerve at the elbow. Posterior interosseous nerve (PIN) entrapment may occur due to prominent radial recurrent artery (RRA), medial edge of the extensor carpi radialis brevis (ECRB), and proximal edge of the supinator muscle (SP) (arcade of Frohse). RN: radial nerve, SRN: superficial radial nerve.
The radial nerve is predisposed to injury and entrapment at several locations along its course, which include the radial nerve in the spiral groove of the humerus (spiral groove syndrome) above the elbow joint, where the PIN travels through the radial tunnel, and the superficial branch of the radial nerve where it crosses over the first dorsal wrist compartment (Wartenberg’s syndrome).
Compression or entrapment of the PIN in the radial tunnel may yield two different clinical presentations: posterior interosseous nerve syndrome and radial tunnel syndrome.
In patients with posterior interosseous nerve syndrome, the clinical presentation includes motor deficits of the extensor muscle group without significant sensory loss.
Patients with radial tunnel syndrome, on the other hand, typically present with pain over the proximal lateral forearm [12, 13], which can be caused by acute trauma, masses, and compression from adjacent structures.

Figure 8: The drawing demonstrates the course of the ulnar nerve from posterior view at the elbow. Note the nerve travels deep to the flexor carpi ulnaris muscle (FCU) beneath the arcuate ligament (AL).
Compressive or entrapped ulnar nerve neuropathies include cubital tunnel syndrome and Guyon’s canal syndrome.
Cubital tunnel syndrome is the second most common peripheral neuropathy of the upper extremity. It may be caused by abnormal fascial bands, subluxation, or dislocation of the ulnar nerve over the medial epicondyle, trauma, or direct compression by soft tissue masses. Clinical symptoms include a sensory abnormality of the ulnar hand and weakness of the flexor carpi muscle group of the 4th and 5th fingers.

Figure 12: The drawing of the median nerve shows that it courses along the anterior elbow, through the two heads of the pronator teres muscle (stars), and into the forearm beneath the edge of the fibrous arch of the flexor digitorum sublimis (open arrow).
Median nerve compression or entrapment neuropathies include pronator syndrome, anterior interosseous syndrome, and carpal tunnel syndrome.
Clinical findings include pain and numbness of the volar aspect of the elbow, forearm, and wrist without muscle weakness.

Figure 14: The drawing shows the proximal course the sciatic nerve passing inferior to the piriformis muscle (PS). SG: superior gemellus muscle.
Sciatic nerve entrapment may occur in the hip region and less commonly in the thigh, and clinical presentations are based upon the level of injury [3]. Sciatic neuropathy may result from conditions such as fibrous or muscular entrapment, vascular compression, scarring related to trauma (Figure 15) or radiation, tumors (Figure 16), and hypertrophic neuropathy [3, 17, 18].

Figure 17: Sagittal oblique projection of the knee illustrates the common peroneal nerve (CPN) arising from the sciatic nerve (SN) at the level of popliteal fossa. It travels around the fibular head deep to the origin of the peroneus longus muscle (PL). TN: tibial nerve.
The etiologies of common peroneal neuropathy may include idiopathic mononeuritis, intrinsic and extrinsic space-occupying lesions including an intraneural ganglion cyst (Figure 18) [21], or traumatic injury of the nerve, especially related to proximal fibular fractures [22]. Clinically, patients may experience pain at the site of entrapment with foot drop and a slapping gait [17, 23].

Figure 19: The drawing of the medial aspect of the ankle showing the course of the tibial nerve (TN) and its branches, the medial calcaneal nerve (MCN), and medial and lateral plantar nerves (MPN and LPN), passing through the tarsal tunnel. FR: flexor retinaculum.
Common etiologies include posttraumatic fibrosis due to fracture, tenosynovitis, ganglion cysts (Figure 20), space-occupying lesions, and dilated or tortuous veins. Most patients with tarsal tunnel syndrome have burning pain and paresthesia along the plantar foot and toes.
Neural Prolotherapy
Denne artikkelen er om en behandlingsform som sprøyter inn dextrose rett under huden for å stimulere nervetrådene der. Den har mange gode forklaringsmodeller om hva som skjer i nervene rett under huden. Nevner bla anterograd og retrograd nervesignaler i C-fibrene. Og Hiltons Law, som er et svært interessant konsept: nervene som går til et ledd går også til musklene som beveger leddet og huden over muskelens feste. Viser til at dextrose hemmer betennelse i nervene, men dette er et vanskelig konsept ved f.eks. diabetisk nevropati hvor hyperglycemi er noe av årsaken til nerveskaden i utgangspunktet. Dog hyperglycemi påvirker blodsirkulasjonen først og fremst.
http://www.orthohealing.com/wp-content/uploads/2011/10/Neural_prolotherapy.pdf
paThology oF NEUrogENiC iNFlaMMaTioN
The pathology of neurogenic inflammation is well established.1, 2, 16 Ligaments, tendons and joints have TRPV1-sensitive C pain fiber innervation. Dr. Pybus explains that the C pain fibers transmit the “deep pain” often seen with osteoarthritis.14 “When these C pain fibers are irritated anywhere along their length they will transmit ectopic impulses in both forward (prodromic) and reverse (antidromic) direction.”14 The forward direction of the nerve signal will cause pain perception as the signal travels through the posterior root ganglia up to the brain. You will also have a local reflex action from the spinal cord ventral horn cells out to the muscle fibers, which will cause a reflex muscle spasm.14 The reverse (antidromic) signal will travel to the blood vessels where substance P is released causing swelling and pain. The nerves themselves also have a nerve supply called the Nervi Nervorum (NN).2 In a pathological state, the NN can release substance P (Sub P) and Calcitonin Gene Related Peptide (CGRP) onto these C pain fibers.11 Sub P and CGRP are known to cause pain, swelling of the nerve and surrounding tissue.7
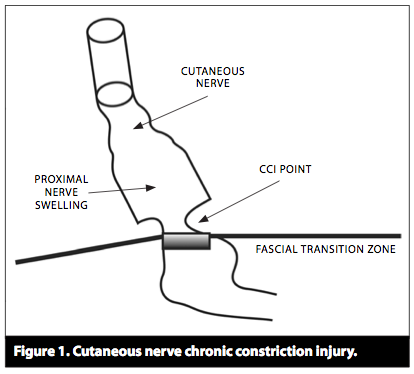
Dr. Lyftogt discussed in his recent Neural Prolotherapy meeting that “Cutaneous nerves pass through many fascial layers on their way to the spine. When there is neurogenic swelling at the Fascial Penetration Zone, a Chronic Constriction Injury (CCI) occurs. The CCI points will inhibit flow of Nerve Growth Factor (NGF).8, 7 Proper flow of NGF is essential for nerve health and repair.”3 (See Figure 1.)
There are two major ways that the fascial penetration point can affect a nerve. Trauma to a nerve will cause edema to travel proximal and distal to the injury. When this swelling reaches the fascial penetration points this can cause a self- strangulation of the nerve and decrease nerve growth factor flow.16, 17 Morton’s neuroma is a clinical example of this.17
Dr. Pybus has also suggested that a change in fascial tension from repetitive muscle dysfunction can also cause a CCI point.15, 17
Another critical concept in NPT is what is called Bystander disease.9, 17 Bystander disease helps explain how superficial nerve pathology can affect deeper anatomic structures.9 This is based on Hilton’s law. Hilton’s law states: the nerve supplying a joint also supplies both the muscles that move the joint and the skin covering the articular insertion of those muscles.9 An example: The musculocutaneous nerve supplies the elbow with pain and proprioception as it is the nerve supply to the biceps brachii and brachialis muscles, as well as the skin close to the insertion of these muscles.17 Hilton’s Law arises as a result of the embryological development of humans.
This concept of Hilton’s law coupled with the idea of anterograde and retrograde axonal flow of neurodegenerative peptides,17 can help explain the wide reaching affects of NPT on pain control.
Glucose responsive nerves have been demonstrated throughout the nervous system.4, 5, 6 One proposed mechanism of action suggests that dextrose binds to pre synaptic calcium channels and inhibits the release of substance P and CGRP, thereby decreasing neurogenic inflammation. This allows normal flow of nerve growth factor and subsequent nerve repair and decreased pain.7

1 Geppetti, et al. Neurogenic Inflammation. Boca Raton: Edited CRC Press; 1996. Chapter 5, Summary; p.53-63.
2 Marshall J. Nerve stretching for the relief or cure of pain. The Lancet.1883;2:1029-36.
8 Bennett GJ, et al. A peripheral mononeuropathy in rat that produces disorders of pain sensation like those seen in man. Pain. 1988;33(1):87-107.
9 Hilton J. On rest and Pain. In Jacobesen WHA(ed): On Rest and Pain, 2nd edition, New York: William Wood & company, 1879.
Scratch collapse test for evaluation of carpal and cubital tunnel syndrome.
Viser hvilken klinisk relevanse scratch collapse test har for å finne hvor nerver er i klem.
http://www.ncbi.nlm.nih.gov/pubmed/18984333
For the new test, the patient resisted bilateral shoulder external rotation with elbows flexed. The area of suspected nerve compression was lightly «scratched,» and then resisted shoulder external rotation was immediately repeated. Momentary loss of shoulder external rotation resistance on the affected side was considered a positive test.
For carpal tunnel syndrome, sensitivities were 64%, 32%, and 44% for the scratch collapse test, Tinel’s test, and wrist flexion/compression test, respectively. For cubital tunnel syndrome, sensitivities were 69%, 54%, and 46% for the scratch collapse test, Tinel test, and elbow flexion/compression test, respectively. The scratch collapse test had the highest negative predictive value (73%) for carpal tunnel syndrome. Tinel’s test had the highest negative predictive value (98%) for cubital tunnel syndrome.
The scratch collapse test had significantly higher sensitivity than Tinel’s test and the flexion/nerve compression test for carpal tunnel and cubital tunnel syndromes. Accuracy for this test was 82% for carpal tunnel syndrome and 89% for cubital tunnel syndrome.
Mer utfyllende studie om Scratch Collapse her: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2880669/
Though the exact mechanism of the scratch collapse test is unknown, we believe it may represent a gross physical manifestation of the “cutaneous silent period.” This EMG-demonstrated phenomenon is observed following noxious stimuli. A brief pause of voluntary muscle contraction is demonstrated following stimulation of a cutaneous nerve [24]. The scratch collapse yields a similar reflex response. We propose that as the nervi-nervorum at the site of neuritis are stimulated, an ipsilateral central inhibition is transiently activated. It is not surprising that this response would be most robust at the focus of the neuritis.
The scratch collapse examination shares several features with the cutaneous silent period. Both phenomena occur after a noxious stimulus, are very resistant to habituation, are able to override voluntary muscle contraction, and result in a deferment in resistance in a pattern that corresponds to the withdrawal of the extremity into a position of protection (e.g., in this case, internally rotating the arms in against the body) [9, 11, 13, 16, 17]. From an evolutionary standpoint, such a reflex would be important in survival.
The test offers an advantage over these other tests in that it appears to precisely localize the site of nerve compression.
Undervisning om nervekompresjon nevropati og kirurgi i armen
Nervekompresjon begynner i en mild variant, hvor myelinlaget rundt nervene fortsatt er tykt og fint. Blodsirkulasjonen hemmes. Smerter og paraestesier kommer og går. Tinels tegn er negativt tidlig i progresjonen. Scratch-Collapse Test viser hvor i nervebanen det er kompresjonproblemer(f.eks. doublecrush syndrome).
Blir moderat, hvor myelinlaget blir tynt. Det blir hevelse i nerven og bindevevet blir tykkere i området. Smerter er konstante og musklene svekkes. Det tar 3-4 mnd å bygge opp myelinlaget igjen når kompresjonen er rettet opp.
Og alvorlig, hvor myelinlaget er borte. Nervetrådene forvinner mer og mer. Atrofi og nummenhet i musklene. Når kompresjonen er borte repareres nerven ca.3 cm i måneden.
http://prezi.com/mjuaxe0cwwbr/?utm_campaign=share&utm_medium=copy&rc=ex0share
