Studie som nevner hvordan «fascial unwinding» skjer ved hjelp av stimulering av mekanoreseptorer i huden. Parasympatikus aktiveres og gjør at muskelspenninger slipper taket.
http://ijtmb.org/index.php/ijtmb/article/view/43/75
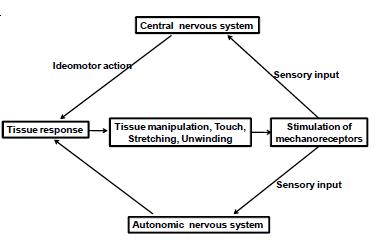
Hypothetical Model: During fascial unwinding, the therapist stimulates mechanoreceptors in the fascia by applying gentle touch and stretching. Touch and stretching induce relaxation and activate the parasympathetic nervous system. They also activate the central nervous system, which is involved in the modulation of muscle tone as well as movement. As a result, the central nervous system is aroused and thereby responds by encouraging muscles to find an easier, or more relaxed, position and by introducing the ideomotor action. Although the ideomotor action is generated via normal voluntary motor control systems, it is altered and experienced as an involuntary response.
Conclusions: Fascial unwinding occurs when a physically induced suggestion by a therapist prompts ideomotor action that the client experiences as involuntary. This action is guided by the central nervous system, which produces continuous action until a state of ease is reached. Consequently, fascial unwinding can be thought of as a neurobiologic process employing the self-regulation dynamic system theory.
In this paper, I propose a model based on scientific literature to explain the process and mechanism of fascial unwinding (Fig. 1). The model is based on the theories of ideomotor action by Carpenter(18) and Dorko,(16) fascia neurobiologic theory by Schleip,(4,5) and the psychology of consciousness by Halligan and Oakley.(19)
A set of conditions are required to initiate or facilitate the unwinding process. The therapist’s sensitivity and fine palpation skills form the most important part of these conditions, but it is also imperative that the client be able to relax and “let go” of his or her body.
In the first stage—the initiation or induction phase— the therapist working on a client will introduce touch or stretching onto the tissue. Touch is the entrance requirement for the process of unwinding. Touch stimulates the fascia’s mechanoreceptors and, in turn, arouses a parasympathetic nervous system response.(5) As a result of this latter response, the client is in a state of deep relaxation and calm, sometimes followed with rapid eye movement, twitching, or deep breathing—a state that can be observed clinically.(20,21) In this state, the conscious mind is relaxed and off guard. Stimulation of mechanoreceptors also influences the central nervous system. The central nervous system responds to this proprioceptive input by allowing the muscles to perform actions that decrease tone or that create movement in a joint or limb, making it move into an area of ease. At this point, ideomotor reflexes occur. Ideomotor action pertains to involuntary muscle movement, which can manifest in various ways and is directed at the central nervous system.(22)
These reflexes occur unconsciously, indicating dissociation between voluntary action and conscious experience.(23) In clinical situations, the client is unaware of the unconscious movement and thinks that it is generated by the therapist. This unconscious movement or stretching sensation stimulates a response in the tissue, providing a feedback to the central nervous system as outlined in the theory of ideomotor action.(24) The process is repeated until the client is relaxed or has reached a “still point” or state of ease.
The indirect stimulation of the autonomic nervous system (that is, the parasympathetic nervous system), which results in global muscle relaxation and a more peaceful state of mind, represents the heart of the changes that are so vital to many manual therapies. Gentler types of myofascial stretching and cranial techniques have also long been acknowledged to affect the parasympathetic nervous system.(25) Bertolucci(20) observed that, when a client is being treated with a muscle repositioning technique, the client begins to show involuntary motor reactions—reactions that include the involuntary action of related muscles and rapid eye movements. Several studies have evaluated the physiologic changes in the autonomic nervous system that occur as a result of craniosacral and MFR interventions,(21,26) clinically-known techniques that can trigger the unwinding process.
Recent studies have used heart rate variability, respiratory rate, skin conductance, and skin temperature as measures of physiologic change. Zullow and Reisman(26) indicated an increase in parasympathetic activity resulting from the compression of the fourth intracranial ventricle (CV4) maneuver and sacral holds, as measured by heart rate variability. Using heart rate variability measurement, Henley et al.(25) demonstrated that cervical MFR shifts sympathovagal balance from the sympathetic to the parasympathetic nervous system.
Dorko(16) was the first to suggest that fascial unwinding can be simply explained as an ideomotor movement. McCarthy et al.(29) were the first to document unwinding as an ideomotor-based manual therapy in the treatment of a patient with chronic neck pain. Their research showed that a reduction in pain intensity and perceived disability can be achieved with the introduction of ideomotor treatment.
A model built upon the neurobiologic, ideomotor action, and consciousness theories is proposed to explain the mechanism of unwinding. Touch, stretching, and manual therapy can induce relaxation in the parasympathetic nervous system. They also activate the central nervous system, which is involved in the modulation of muscle tone as well as movement. This activation stimulates the response to stretching: muscles find areas and positions of ease, the client experiences less pain or is more relaxed, thereby introducing the ideomotor action. The ideomotor action is generated through normal voluntary motor control systems, but is altered and experienced as an involuntary reaction. The stretching sensation provides a feedback to the nervous system, which in turn will generate the movements again.

